

Development and validation of models predicting treatment patterns in women with urinary urgency and/or urgency incontinence: A Symptoms of Lower Urinary Tract Dysfunction Research Network observational cohort study
- PMID: 37269483
- PMCID: PMC10581676
- DOI: 10.1002/nau.25222
Development and validation of models predicting treatment patterns in women with urinary urgency and/or urgency incontinence: A Symptoms of Lower Urinary Tract Dysfunction Research Network observational cohort study
Abstract
Purpose: To develop a tool to predict a woman's treatment pattern for bothersome urinary urgency (UU) and/or UU incontinence over 1 year after presenting for care at urology or urogynecology clinics.
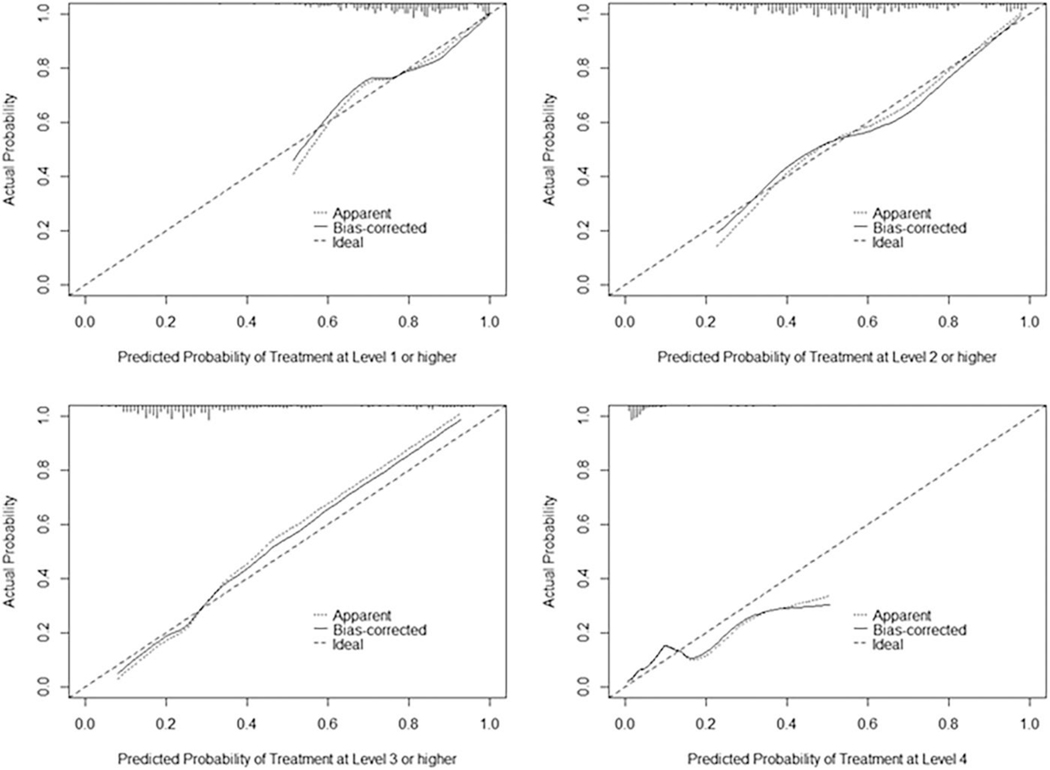
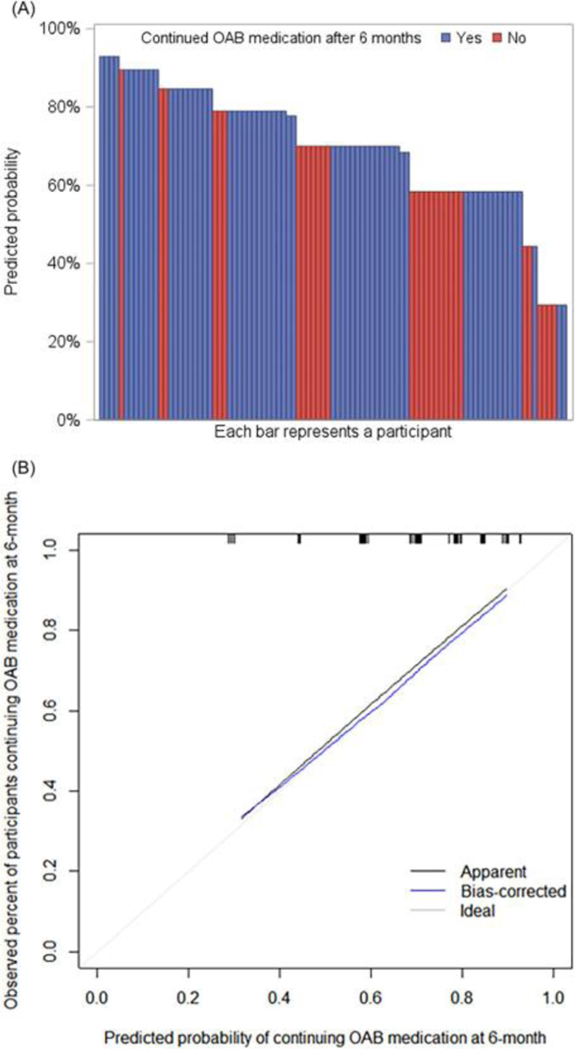
Methods: The Symptoms of Lower Urinary Tract Dysfunction Research Network observational cohort study enrolled adult women with bothersome UU and/or UU incontinence using the lower urinary tract symptoms (LUTS) Tool who were seeking care for LUTS. Treatments for UU and/or urgency incontinence were ordered from least to most invasive. Ordinal logistic and Cox proportional hazard regression models were fit to predict the most invasive level of treatment during follow-up and overactive bladder (OAB) medication discontinuation, respectively. Binary logistic regression was performed to predict sling treatment during the study follow-up. Clinical tools were then created using the models listed above to predict treatment pattern over 12 months.
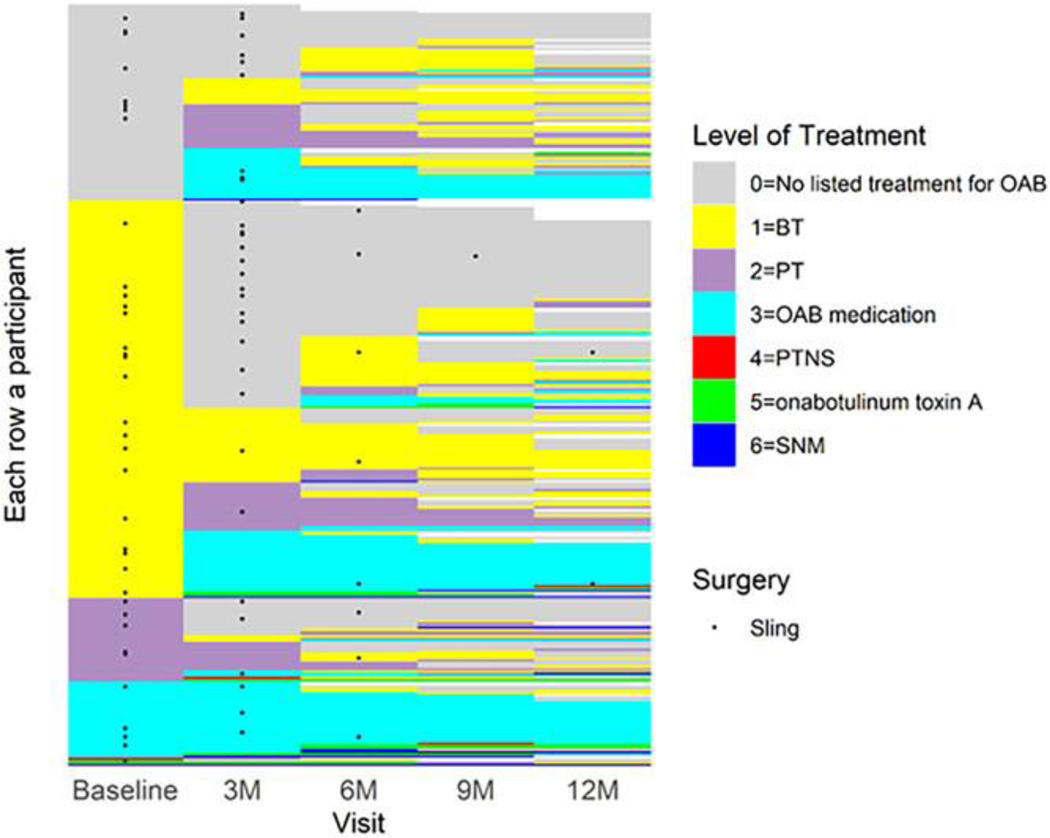
Results: Among 349 women, 281 reported UU incontinence, and 68 reported UU at baseline. The highest level of treatment during the study was as follows: 20% no treatment, 24% behavioral treatments, 23% physical therapy, 26% OAB medication, 1% percutaneous tibial nerve stimulation, 3% onabotulinumtoxin A, and 3% sacral neuromodulation. Slings were placed in 10% (n = 36) of participants before baseline and in 11% (n = 40) during study follow-up. Baseline factors associated with predicting the most invasive level of treatment included baseline level of treatment, hypertension, UU incontinence severity, stress urinary incontinence (SUI) severity, and anticholinergic burden score. Less severe baseline depression and less severe UU incontinence were associated with OAB medication discontinuation. UU and SUI severity were associated with sling placement during the study period. Three tools are available to predict: (1) highest level of treatment; (2) OAB medication discontinuation; and (3) sling placement.
Conclusions: OAB treatment prediction tools developed in this study can help providers individualize treatment plans and identify not only patients at risk for treatment discontinuation but also patients who may not be escalated to potentially beneficial OAB treatments, with the goal to improve clinical outcomes for patients suffering from this chronic and often debilitating condition.
Keywords: overactive bladder; treatment; urgency urinary incontinence; urinary urgency.
© 2023 The Authors. Neurourology and Urodynamics published by Wiley Periodicals LLC.
Conflict of interest statement
Conflicts of Interest
The authors declare no conflicts of interest.
Figures
Similar articles
-
Treatment patterns in women with urinary urgency and/or urgency urinary incontinence in the symptoms of Lower Urinary Tract Dysfunction Research Network Observational Cohort Study.Neurourol Urodyn. 2023 Jan;42(1):194-204. doi: 10.1002/nau.25067. Epub 2022 Oct 23. Neurourol Urodyn. 2023. PMID: 36579974 Free PMC article.
-
Overactive bladder symptoms after midurethral sling surgery in women: Risk factors and management.Neurourol Urodyn. 2018 Jan;37(1):83-88. doi: 10.1002/nau.23328. Epub 2017 Jun 20. Neurourol Urodyn. 2018. PMID: 28631830 Review.
-
Effect of extracorporeal magnetic energy stimulation on bothersome lower urinary tract symptoms and quality of life in female patients with stress urinary incontinence and overactive bladder.J Obstet Gynaecol Res. 2013 Nov;39(11):1526-32. doi: 10.1111/jog.12090. Epub 2013 Jul 15. J Obstet Gynaecol Res. 2013. PMID: 23855601
-
Overactive bladder (OAB): A symptom in search of a disease - Its relationship to specific lower urinary tract symptoms and conditions.J Pediatr Urol. 2017 Jun;13(3):277.e1-277.e4. doi: 10.1016/j.jpurol.2017.02.010. Epub 2017 Mar 10. J Pediatr Urol. 2017. PMID: 28527720
-
What Are the Short-term Benefits and Potential Harms of Therapeutic Modalities for the Management of Overactive Bladder Syndrome in Women? A Review of Evidence Under the Auspices of the European Association of Urology, Female Non-neurogenic Lower Urinary Tract Symptoms Guidelines Panel.Eur Urol. 2023 Sep;84(3):302-312. doi: 10.1016/j.eururo.2023.05.014. Epub 2023 Jun 17. Eur Urol. 2023. PMID: 37331921 Review.
References
-
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003;61(1):37–49. - PubMed
-
- Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4–20. - PubMed
-
- Brown MT, Bussell J, Dutta S, Davis K, Strong S, Mathew S. Medication adherence: Truth and consequences. Am J Med Sci. 2016;351(4):387–399. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
