

Health-related quality of life and pain outcomes with [177Lu]Lu-PSMA-617 plus standard of care versus standard of care in patients with metastatic castration-resistant prostate cancer (VISION): a multicentre, open-label, randomised, phase 3 trial
- PMID: 37269841
- PMCID: PMC10641914
- DOI: 10.1016/S1470-2045(23)00158-4
Health-related quality of life and pain outcomes with [177Lu]Lu-PSMA-617 plus standard of care versus standard of care in patients with metastatic castration-resistant prostate cancer (VISION): a multicentre, open-label, randomised, phase 3 trial
Abstract
Background: In VISION, the prostate-specific membrane antigen (PSMA)-targeted radioligand therapy lutetium-177 [177Lu]Lu-PSMA-617 (vipivotide tetraxetan) improved radiographic progression-free survival and overall survival when added to protocol-permitted standard of care in patients with metastatic castration-resistant prostate cancer. Here, we report additional health-related quality of life (HRQOL), pain, and symptomatic skeletal event results.
Methods: This multicentre, open-label, randomised, phase 3 trial was conducted at 84 cancer centres in nine countries in North America and Europe. Eligible patients were aged 18 years or older; had progressive PSMA-positive metastatic castration-resistant prostate cancer; an Eastern Cooperative Oncology Group (ECOG) performance status score of 0-2; and had previously received of at least one androgen receptor pathway inhibitor and one or two taxane-containing regimens. Patients were randomly assigned (2:1) to receive either [177Lu]Lu-PSMA-617 plus protocol-permitted standard of care ([177Lu]Lu-PSMA-617 group) or standard of care alone (control group) using permuted blocks. Randomisation was stratified by baseline lactate dehydrogenase concentration, liver metastases, ECOG performance status, and androgen receptor pathway inhibitor inclusion in standard of care. Patients in the [177Lu]Lu-PSMA-617 group received intravenous infusions of 7·4 gigabecquerel (GBq; 200 millicurie [mCi]) [177Lu]Lu-PSMA-617 every 6 weeks for four cycles plus two optional additional cycles. Standard of care included approved hormonal treatments, bisphosphonates, and radiotherapy. The alternate primary endpoints were radiographic progression-free survival and overall survival, which have been reported. Here we report the key secondary endpoint of time to first symptomatic skeletal event, and other secondary endpoints of HRQOL assessed with the Functional Assessment of Cancer Therapy-Prostate (FACT-P) and EQ-5D-5L, and pain assessed with the Brief Pain Inventory-Short Form (BPI-SF). Patient-reported outcomes and symptomatic skeletal events were analysed in all patients who were randomly assigned after implementation of measures designed to reduce the dropout rate in the control group (on or after March 5, 2019), and safety was analysed according to treatment received in all patients who received at least one dose of treatment. This trial is registered with ClinicalTrials.gov, NCT03511664, and is active but not recruiting.
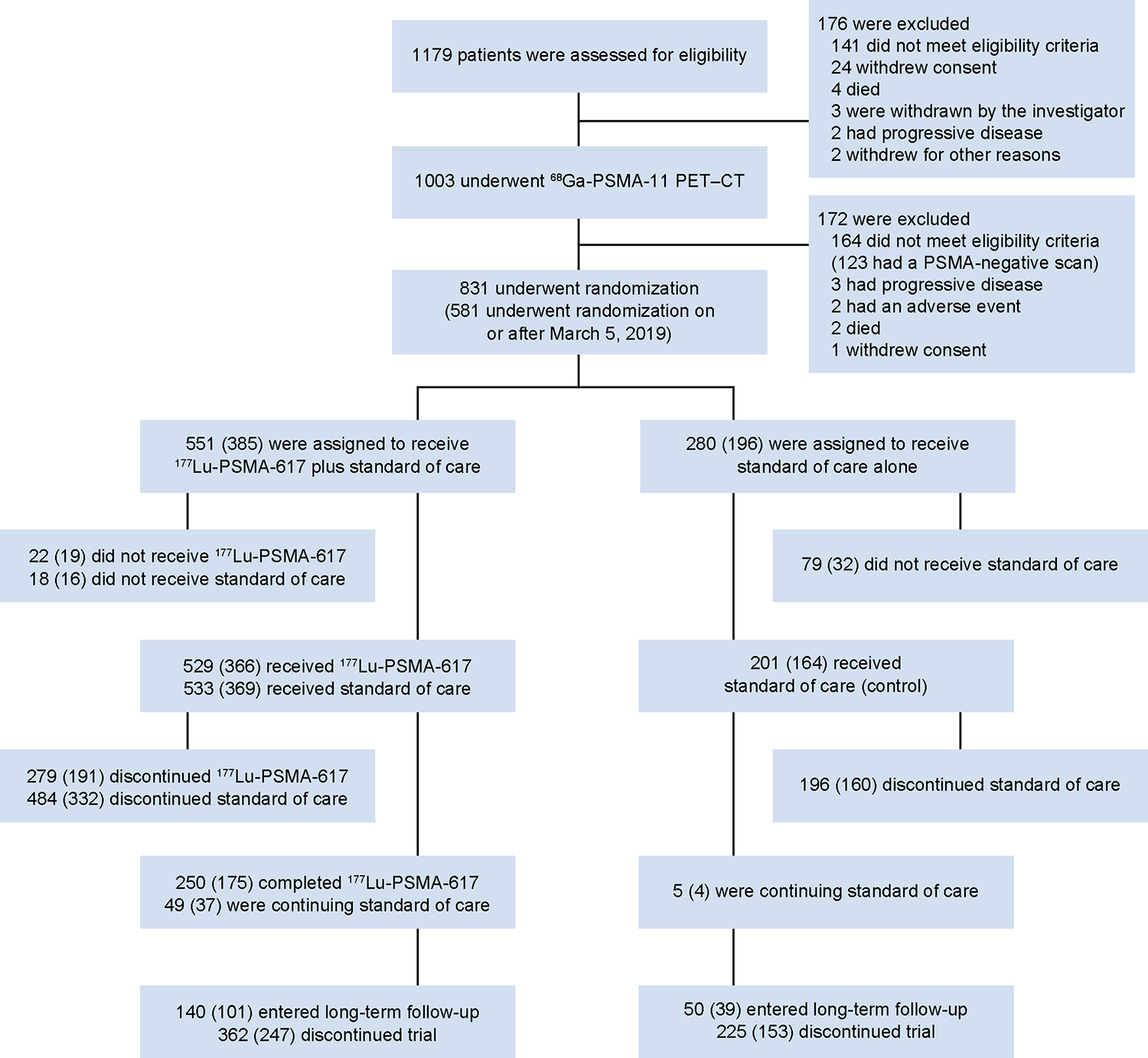
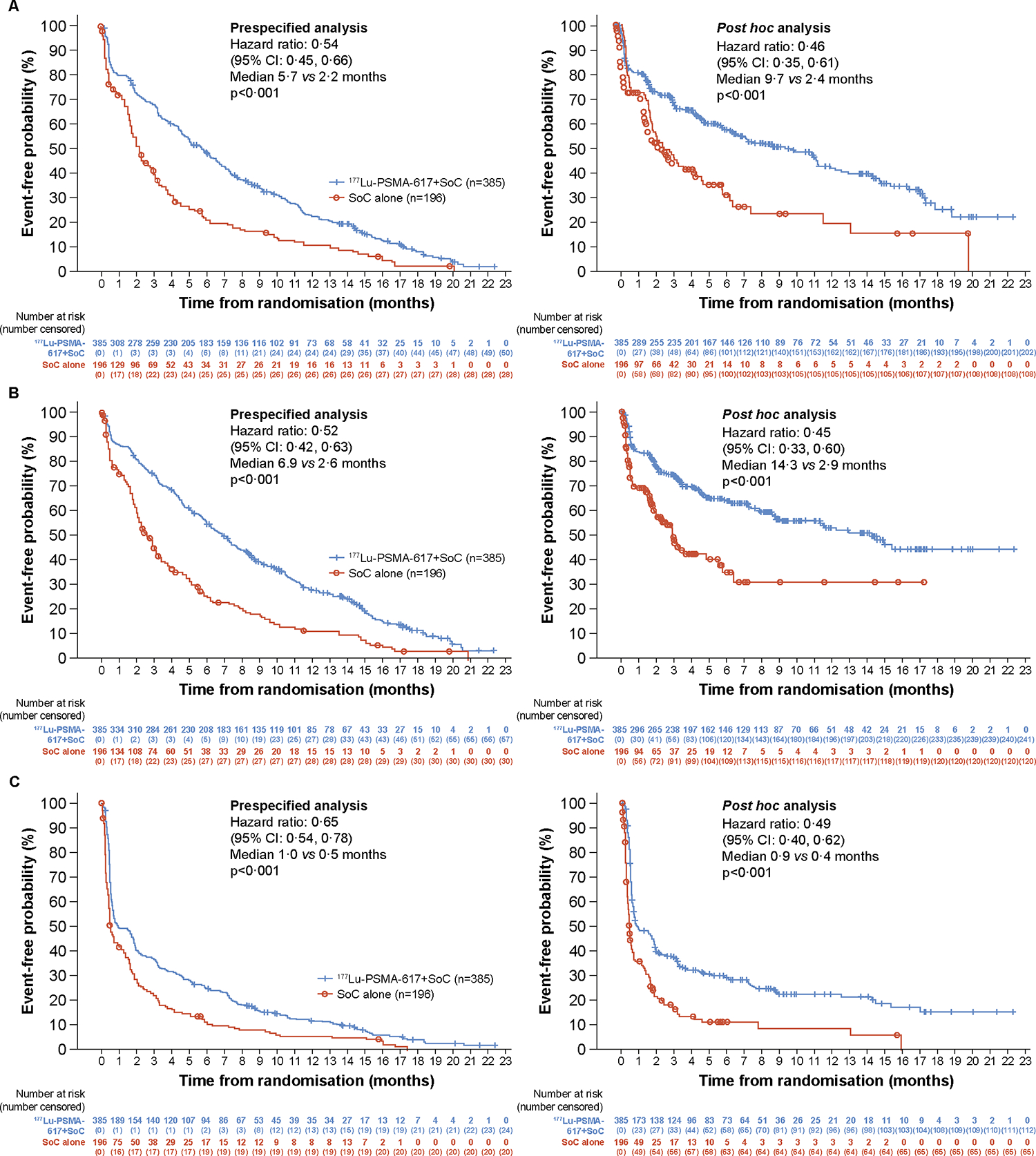
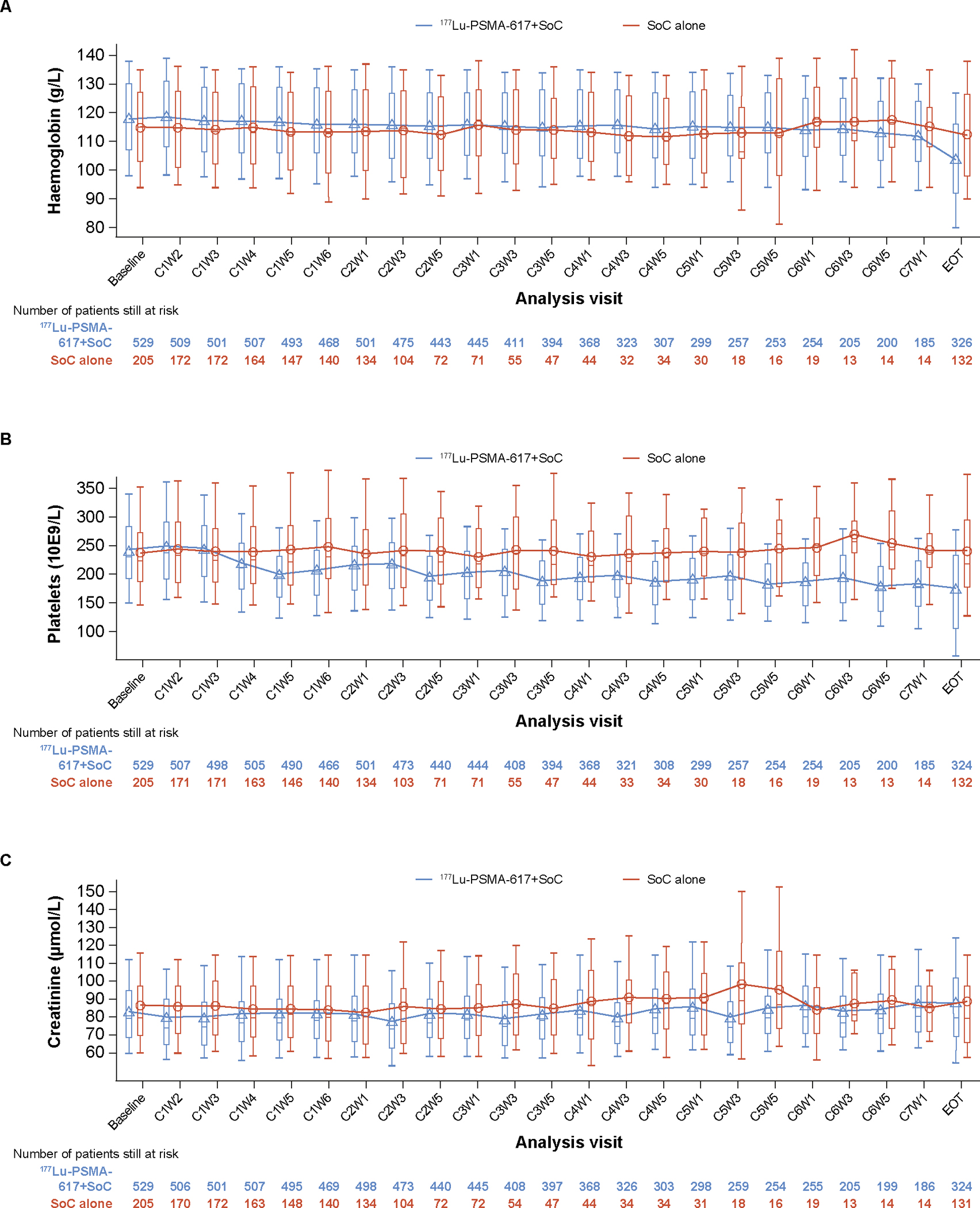
Findings: Between June 4, 2018, and Oct 23, 2019, 831 patients were enrolled, of whom 581 were randomly assigned to the [177Lu]Lu-PSMA-617 group (n=385) or control group (n=196) on or after March 5, 2019, and were included in analyses of HRQOL, pain, and time to first symptomatic skeletal event. The median age of patients was 71 years (IQR 65-75) in the [177Lu]Lu-PSMA-617 group and 72·0 years (66-76) in the control group. Median time to first symptomatic skeletal event or death was 11·5 months (95% CI 10·3-13·2) in the [177Lu]Lu-PSMA-617 group and 6·8 months (5·2-8·5) in the control group (hazard ratio [HR] 0·50, 95% CI 0·40-0·62). Time to worsening was delayed in the [177Lu]Lu-PSMA-617 group versus the control group for FACT-P score (HR 0·54, 0·45-0·66) and subdomains, BPI-SF pain intensity score (0·52, 0·42-0·63), and EQ-5D-5L utility score (0·65, 0·54-0·78). Grade 3 or 4 haematological adverse events included decreased haemoglobin (80 [15%] of 529 assessable patients who received [177Lu]Lu-PSMA-617 plus standard of care vs 13 [6%] of 205 who received standard of care only), lymphocyte concentrations (269 [51%] vs 39 [19%]), and platelet counts (49 [9%] vs five [2%]). Treatment-related adverse events leading to death occurred in five (1%) patients who received [177Lu]Lu-PSMA-617 plus standard of care (pancytopenia [n=2], bone marrow failure [n=1], subdural haematoma [n=1], and intracranial haemorrhage [n=1]) and no patients who received standard of care only.
Interpretation: [177Lu]Lu-PSMA-617 plus standard of care delayed time to worsening in HRQOL and time to skeletal events compared with standard of care alone. These findings support the use of [177Lu]Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer who received previous androgen receptor pathway inhibitor and taxane treatment.
Funding: Advanced Accelerator Applications (Novartis).
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests KF reports consultant or advisory fees from Janssen, Bayer, Astellas, Sanofi, Orion Pharma, CureVac, AstraZeneca, ESSA Pharma, Amgen, Bristol Myers Squibb, Clovis Oncology, Lilly, Novartis, Daiichi-Sankyo, Pfizer, and MSD. KH reports consultant or advisory fees from ABX, AstraZeneca, Advanced Accelerator Applications (Novartis), Aktis Oncology, Amgen, Bayer, BTG, Curium, Debiopharm, Endocyte, GE HealthCare, Janssen, Ipsen, Novartis, Pharma15, Siemens Healthineers, Sirtex Medical, SOFIE Biosciences, Theragnostics, and Y-mAbs Therapeutics. BJK reports consultant or advisory fees from Advanced Accelerator Applications (Novartis), Astellas, Bayer, Janssen, Terumo, PSFI, and Isotope Technologies Munich; and research funding from Advanced Accelerator Applications (Novartis). KR reports consulting or advisory fees from ABX-CRO, ABX, Advanced Accelerator Applications (Novartis), and Bayer. KNC reports consultant or advisory fees from AstraZeneca, ESSA Pharma, Janssen, Merck, POINT Biopharma, and Roche; and research funding from AstraZeneca, ESSA Pharma, Janssen, Merck, POINT Biopharma, Novartis, Roche, and Arvinas. MJM reports consultant or advisory fees from Exelixis, Lanctheus, AstraZeneca, Amgen, Daiichi, Convergent Therapeutics, Clarity Pharmaceuticals, Pfizer, Blue Earth Diagnostics, and Isotope Technologies Munich; and research funding from Novartis. OS reports consultant or advisory fees from Advanced Accelerator Applications (Novartis), Astellas, AstraZeneca, Bayer, Blue Earth Diagnostics, Bavarian Nordic, Bristol Myers Squibb, Clarity Pharmaceuticals, Clovis Oncology, Constellation, Dendreon, EMD Serono, Fusion, Isotope Technologies Munich, Merck, Janssen, Myovant, Myriad, Noria Therapeutics, NorthStar, Novartis, Noxopharm, Progenics, POINT Biopharma, Pfizer, Sanofi, Tenebio, Telix, and Theragnostics; research funding from Bayer, Endocyte, Merck, InVitae, Constellation, Amgen, Advanced Accelerator Applications (Novartis), Arvinas, AstraZeneca, Dendreon, Janssen, Lantheus, Tenebio, and Progenics; holds an issued US patent (number 7 166 691); and owns stock in Lilly, GlaxoSmithKline, AbbVie, Cardinal Health, UnitedHealth Group, Clarity Pharmaceuticals, Noria Therapeutics, and Clovis Oncology. STT reports consultant or advisory fees from Sanofi, Medivation, Astellas, Janssen, Genentech, Bayer, Eisai, Abbvie, Tolmar, Seattle Genetics, Amgen, Clovis Oncology, Pfizer, Novartis, Clarity Pharmaceuticals, Genomic Health, POINT Biopharma, Blue Earth Diagnostics, Aikido, Telix, Convergent Therapeutics, EMD Serono, Myovant, and Merck; research funding from Sanofi, Medivation, Astellas, Janssen, Amgen, Genentech, Newlink, Bristol-Myers Squibb, Inovio, AstraZeneca, Aveo, Rexahn, Bayer, Merck, Abbvie, Karyopharm, Endocyte, Clovis Oncology, Seattle Genetics, Novartis, Gilead, and POINT Biopharma; holds a patent pending with Gilead; and owns stock in Alkido. NV reports consultant or advisory fees from Genzyme, MSD, Janssen, Eisai, AstraZeneca, Dendreon, Pfizer, Bayer, Seagen, Clovis Oncology, Advanced Accelerator Applications (Novartis), and Amgen. JC reports consultant or advisory fees from Astellas, Blue Earth Diagnostics, Curium, DS Pharma, GE Healthcare, Isoray, Janssen, Lightpoint Medical, Lantheus, POINT Biopharma, Radiomedix, IBA RadioPharma, Monrol, Novartis, Telix, and Sanofi; and research funding from Lantheus, Novartis, and POINT Biopharma. JN reports consultant or advisory fees from Curium, POINT Biopharma, Bayer, and Pfizer; and research funding from Advanced Accelerator Applications (Novartis) and ABX. ATK and XXW report consultant or advisory fees from Advanced Accelerator Applications (Novartis). VSK reports consultant or advisory fees from Clovis Oncology, Pfizer, EMD Serono, Seagen, AstraZeneca, Janssen, Astellas, Seattle Genetics, Dendreon, Guidepoint, GLG, and ExpertConnect; and research funding from Janssen, Clovis Oncology, Nektar, Taiho, Merck, and Advanced Accelerator Applications (Novartis). JdB reports consultant or advisory fees from AstraZeneca, Astellas, Bayer, Cell Centric, Daiichi, Genentech (Roche), Endocyte, Advanced Accelerator Applications (Novartis), Pfizer, GSK, Janssen, Merck Serono, MSD, Sanofi Aventis, and Pfizer; and research funding from AstraZeneca, Bayer, CellCentric, Daiichi, GSK, Harpoon, Janssen, Merck Serono, MSD, Pfizer, Sanofi Aventis, and Genentech (Roche). RG, MD, and RAM are employees or own Novartis stocks and shares. J-MB and BC declare no competing interests.
Figures
References
-
- Sartor O, de Bono JS. Metastatic prostate cancer. N Engl J Med 2018; 378: 645–57. - PubMed
-
- Nuhn P, De Bono JS, Fizazi K, et al. Update on systemic prostate cancer therapies: management of metastatic castration-resistant prostate cancer in the era of precision oncology. Eur Urol 2019; 75: 88–99. - PubMed
-
- Gillessen S, Armstrong A, Attard G, et al. Management of patients with advanced prostate cancer: report from the Advanced Prostate Cancer Consensus Conference 2021. Eur Urol 2022; 82: 115–41. - PubMed
-
- Smith M, De Bono J, Sternberg C, et al. Phase III study of cabozantinib in previously treated metastatic castration-resistant prostate cancer: COMET-1. J Clin Oncol 2016; 34: 3005–13. - PubMed
-
- McKay R, Haider B, Duh MS, et al. Impact of symptomatic skeletal events on health-care resource utilization and quality of life among patients with castration-resistant prostate cancer and bone metastases. Prostate Cancer Prostatic Dis 2017; 20: 276–82. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
