

Pulseless electrical activity and asystole during in-hospital cardiac arrest: Disentangling the 'nonshockable' rhythms
- PMID: 37270088
- PMCID: PMC10527285
- DOI: 10.1016/j.resuscitation.2023.109857
Pulseless electrical activity and asystole during in-hospital cardiac arrest: Disentangling the 'nonshockable' rhythms
Abstract
Background: Pulseless electrical activity (PEA) and asystole account for 81% of initial in-hospital cardiac arrest (IHCA) rhythms in the U.S.A. These "non-shockable" rhythms are often grouped together in resuscitation research and practice. We hypothesized that PEA and asystole are distinct initial IHCA rhythms with distinguishing features.
Methods: This was an observational cohort study using the prospectively collected nationwide Get With The Guidelines®-Resuscitation registry. Adult patients with an index IHCA and an initial rhythm of PEA or asystole between the years of 2006 and 2019 were included. Patients with PEA vs. asystole were compared with respect to pre-arrest characteristics, resuscitation practice, and outcomes.
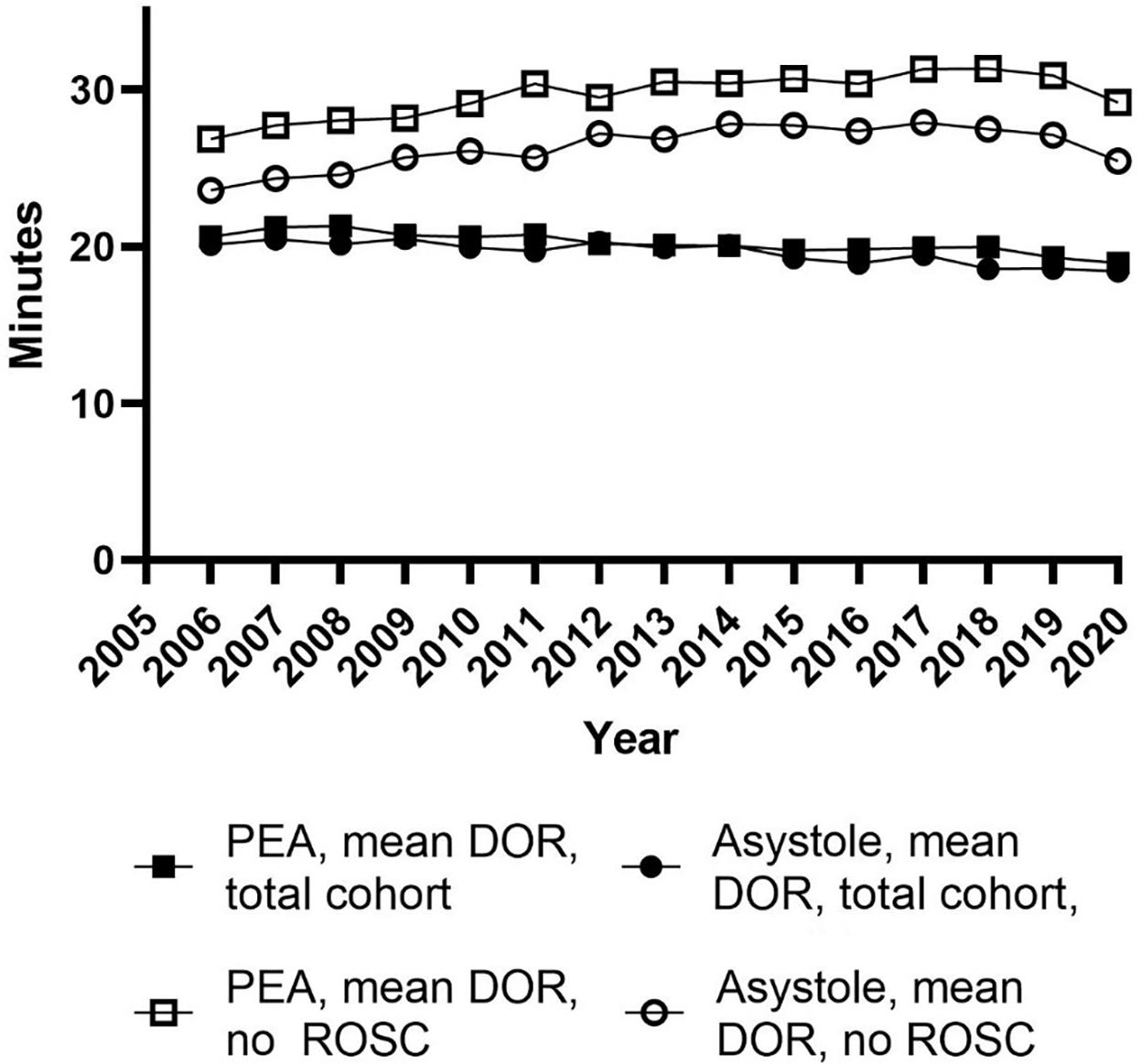
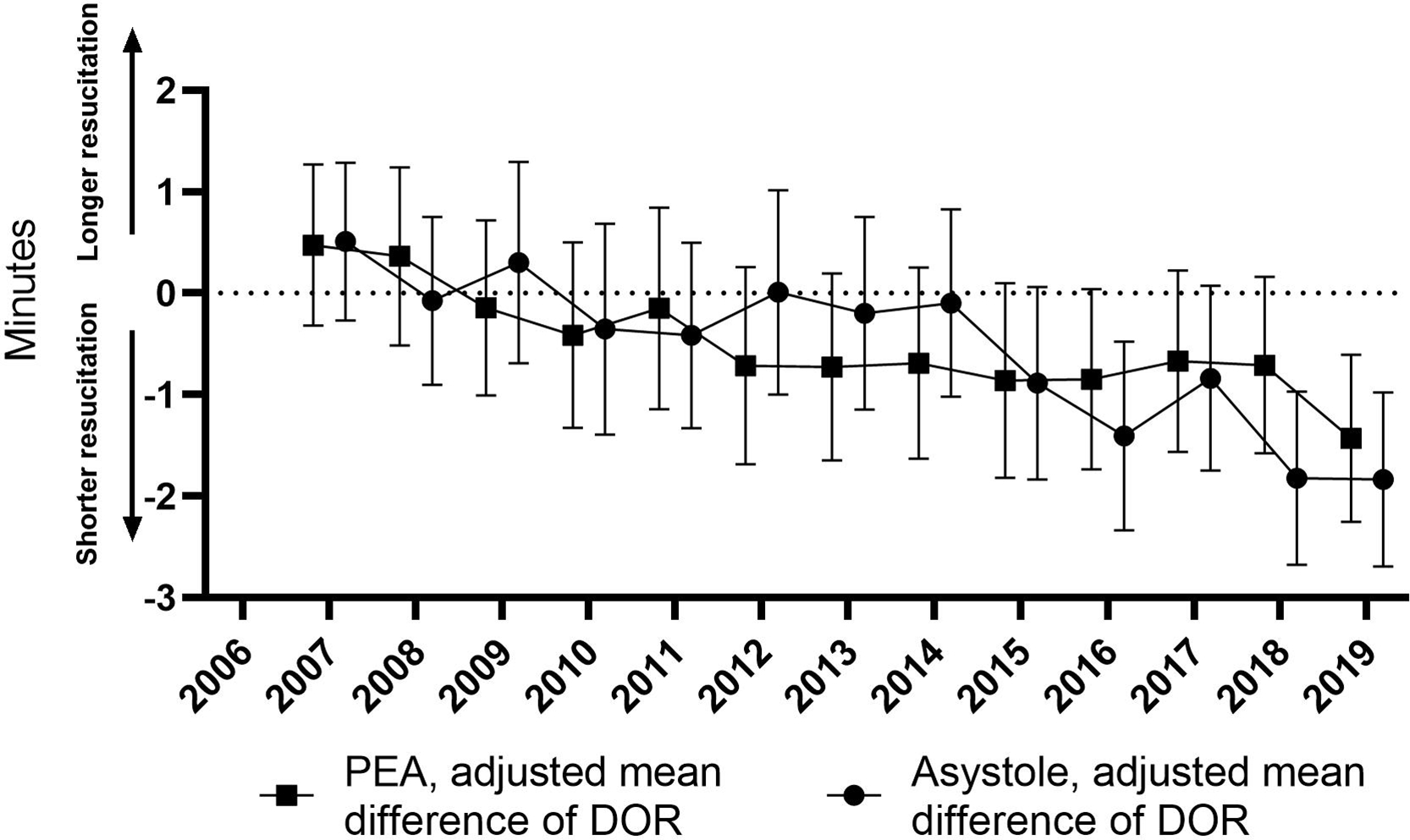
Results: We identified 147,377 (64.9%) PEA and 79,720 (35.1%) asystolic IHCA. Asystole had more arrests in non-telemetry wards (20,530/147,377 [13.9%] PEA vs. 17,618/79,720 [22.1%] asystole). Asystole had 3% lower adjusted odds of ROSC (91,007 [61.8%] PEA vs. 44,957 [56.4%] asystole, aOR 0.97, 95%CI 0.96-0.97, P < 0.01); there was no statistically significant difference in survival to discharge (28,075 [19.1%] PEA vs. 14,891 [18.7%] asystole, aOR 1.00, 95%CI 1.00-1.01, P = 0.63). Duration of resuscitation for those without ROSC were shorter for asystole (29.8 [±22.5] minutes in PEA vs. 26.2 [±21.5] minutes in asystole, adjusted mean difference -3.05 95%CI -3.36--2.74, P < 0.01).
Interpretation: Patients suffering IHCA with an initial PEA rhythm had patient and resuscitation level differences from those with asystole. PEA arrests were more common in monitored settings and received longer resuscitations. Even though PEA was associated with higher rates of ROSC, there was no difference in survival to discharge.
Keywords: Cardiac arrest; Cardiac rhythm; Resuscitation.
Copyright © 2023 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. Jama. 2006;295(1):50–57. - PubMed
-
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart Disease and Stroke Statistics—2018 Update: A Report From the American Heart Association. Circulation. 2018;137(12):e67–e492. - PubMed
-
- Soar J, Nolan JP, Böttiger BW, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resuscitation. 2015;95:100–147. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
