

Central-line associated bloodstream infections in intensive care units before and after implementation of daily antiseptic bathing with chlorhexidine or octenidine: a post-hoc analysis of a cluster-randomised controlled trial
- PMID: 37270604
- PMCID: PMC10239202
- DOI: 10.1186/s13756-023-01260-w
Central-line associated bloodstream infections in intensive care units before and after implementation of daily antiseptic bathing with chlorhexidine or octenidine: a post-hoc analysis of a cluster-randomised controlled trial
Abstract
Backgrounds: Antiseptic bathing did not reduce central-line (CL) associated bloodstream infection (CLABSI) rates in intensive care units (ICU) according to a recent cluster randomised controlled trial (cRCT). However, this analysis did not consider baseline infection rates. Our post-hoc analysis of this cRCT aimed to use a before-after comparison to examine the effect of daily bathing with chlorhexidine, octenidine or water and soap (control) on ICU-attributable CLABSI rates.
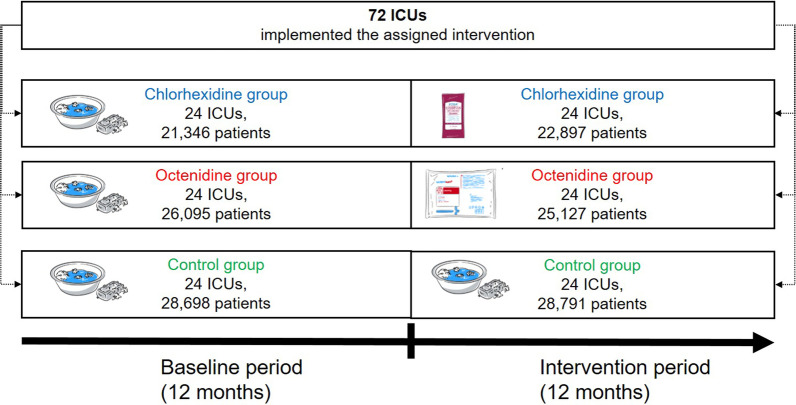
Methods: A post-hoc analysis of a multi-center cRCT was done. ICUs that did not yet perform routine antiseptic bathing were randomly assigned to one of three study groups applying daily bathing with 2% chlorhexidine-impregnated cloths, 0.08% octenidine wash mitts or water and soap (control) for 12 months. Baseline data was assessed 12 months before the intervention started when all ICUs routinely used water and soap. Poisson regression and generalised estimating equation models were applied to identify changes of CLABSI rates per 1000 CL days between intervention and baseline periods in each study group.
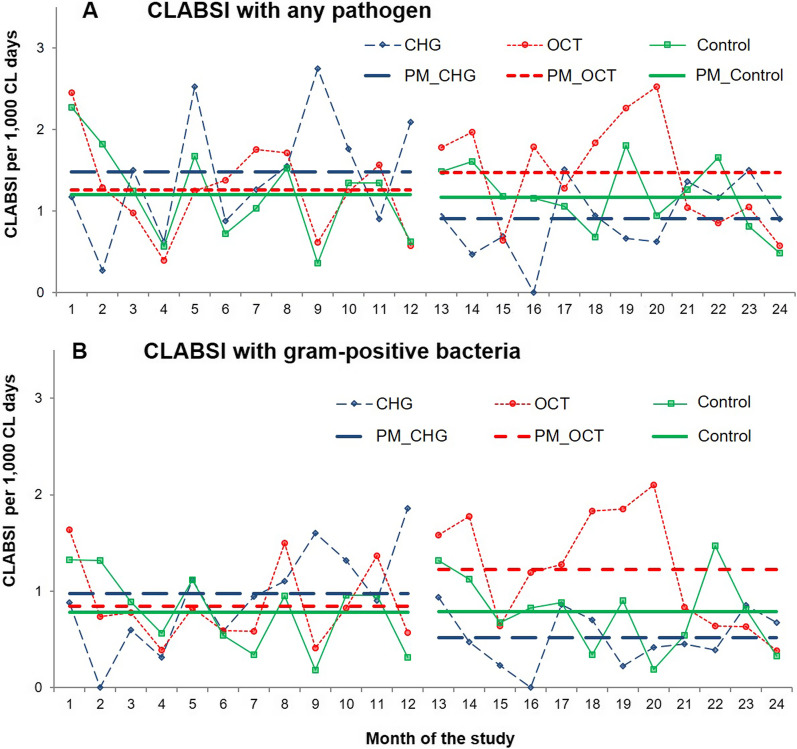
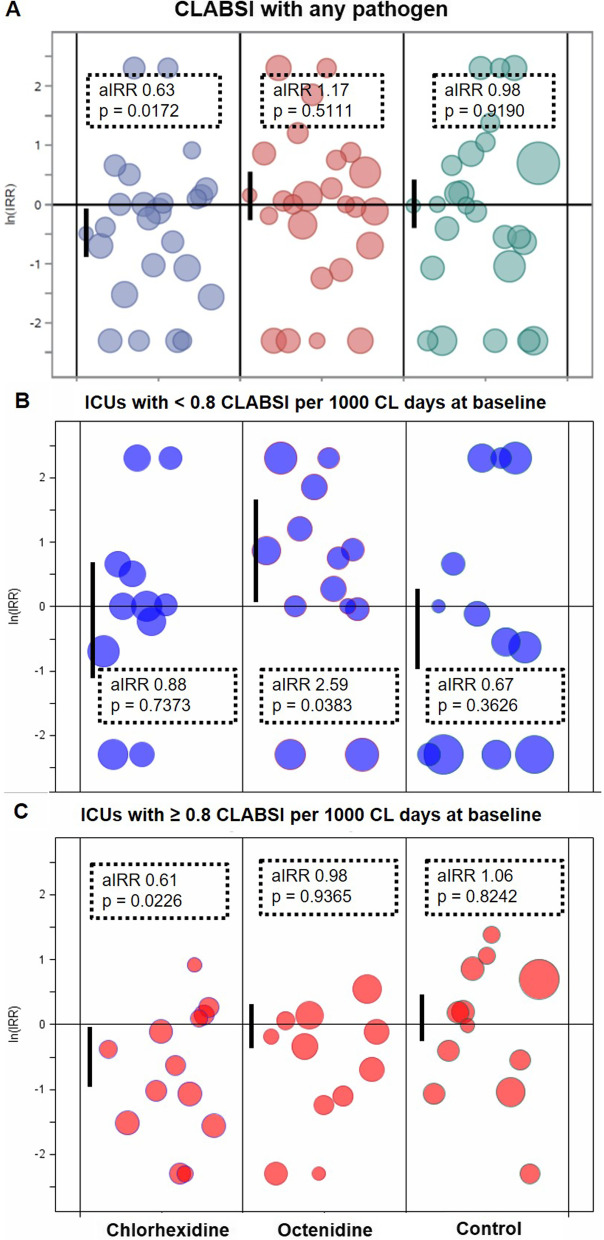
Results: The cRCT was conducted in 72 ICUs (24 per study group) including 76,139 patients in the baseline and 76,815 patients in the intervention period. In the chlorhexidine group, incidence density of CLABSI was reduced from 1.48 to 0.90 CLABSI per 1000 CL days comparing baseline versus intervention period (P = 0.0085). No reduction was observed in the octenidine group (1.26 versus 1.47 CLABSI per 1000 CL days, P = 0.8735) and the control group (1.20 versus 1.17, P = 0.3298). Adjusted incidence rate ratios (intervention versus baseline) were 0.63 (95%CI 0.46-0.87, P = 0.0172) in the chlorhexidine, 1.17 (95% CI 0.79-1.72, P = 0.5111) in the octenidine and 0.98 (95% CI 0.60-1.58, P = 0.9190) in the control group. Chlorhexidine bathing reduced CLABSI with gram-positive bacteria, mainly coagulase-negative staphylococci (CoNS).
Conclusions: In this post-hoc analysis of a cRCT, the application of 2% chlorhexidine-impregnated cloths reduced ICU-attributable CLABSI. This preventive effect of chlorhexidine was restricted to CLABSI caused by gram-positive pathogens (CoNS). In contrast, 0.08% octenidine wash mitts did not reduce CLABSI rates in ICUs. Trial registration Registration number DRKS00010475, registration date August 18, 2016.
Keywords: Antiseptic bathing; CLABSI; Chlorhexidine gluconate; Octenidine dihydrochloride; Post-hoc before-after analysis.
© 2023. The Author(s).
Conflict of interest statement
All authors have no conflicts of interest to declare. On behalf of all authors, the corresponding author states that there is no conflict of interest. The German Ministry of Education and Research (funder) and companies (Sage Products/Stryker, Schülke) funding products and the investigation of tolerances of bacterial isolates to chlorhexidine and octenidine by an independent laboratory had no role in study design, data collection and analysis, data interpretation, the decision to publish, or the preparation of the manuscript.
Figures
References
-
- Vernon MO, Hayden MK, Trick WE, Hayes RA, Blom DW, Weinstein RA. Chlorhexidine gluconate to cleanse patients in a medical intensive care unit: the effectiveness of source control to reduce the bioburden of vancomycin-resistant enterococci. Arch Intern Med. 2006;166(3):306–312. doi: 10.1001/archinte.166.3.306. - DOI - PubMed
-
- Frost SA, Alogso MC, Metcalfe L, Lynch JM, Hunt L, Sanghavi R, et al. Chlorhexidine bathing and health care-associated infections among adult intensive care patients: a systematic review and meta-analysis. Crit Care (London, England) 2016;20(1):379. doi: 10.1186/s13054-016-1553-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
