

Preoperative Treatment of Locally Advanced Rectal Cancer
- PMID: 37272534
- PMCID: PMC10775881
- DOI: 10.1056/NEJMoa2303269
Preoperative Treatment of Locally Advanced Rectal Cancer
Abstract
Background: Pelvic radiation plus sensitizing chemotherapy with a fluoropyrimidine (chemoradiotherapy) before surgery is standard care for locally advanced rectal cancer in North America. Whether neoadjuvant chemotherapy with fluorouracil, leucovorin, and oxaliplatin (FOLFOX) can be used in lieu of chemoradiotherapy is uncertain.
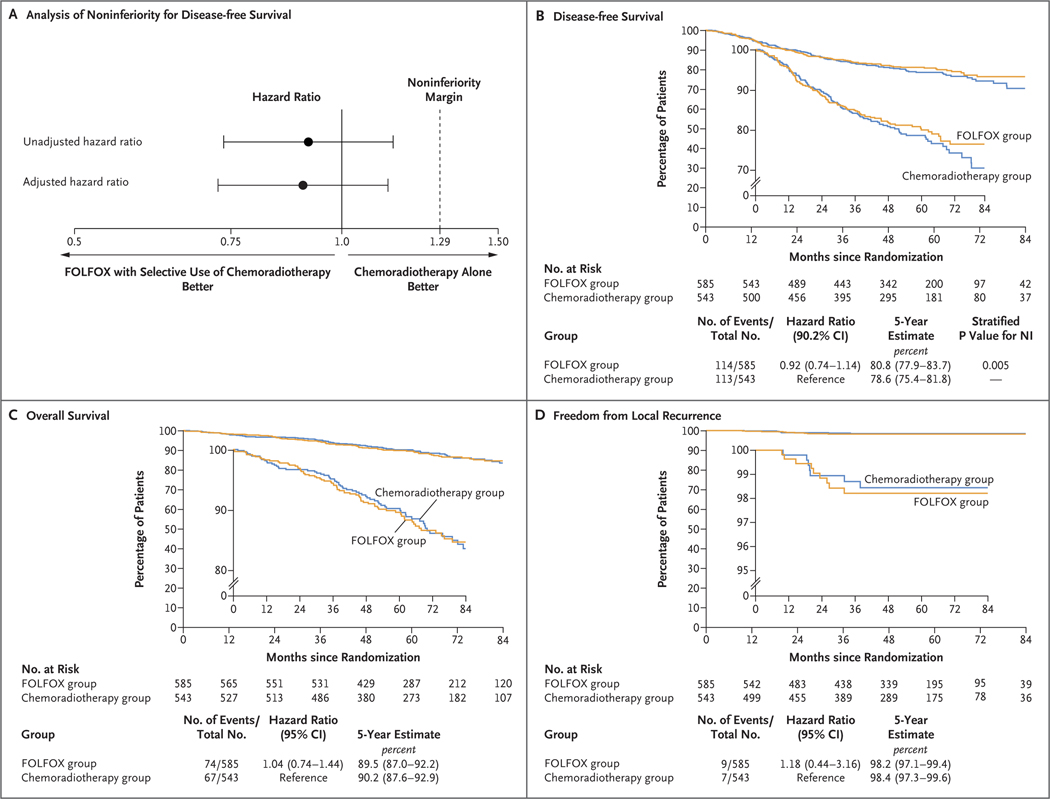
Methods: We conducted a multicenter, unblinded, noninferiority, randomized trial of neoadjuvant FOLFOX (with chemoradiotherapy given only if the primary tumor decreased in size by <20% or if FOLFOX was discontinued because of side effects) as compared with chemoradiotherapy. Adults with rectal cancer that had been clinically staged as T2 node-positive, T3 node-negative, or T3 node-positive who were candidates for sphincter-sparing surgery were eligible to participate. The primary end point was disease-free survival. Noninferiority would be claimed if the upper limit of the two-sided 90.2% confidence interval of the hazard ratio for disease recurrence or death did not exceed 1.29. Secondary end points included overall survival, local recurrence (in a time-to-event analysis), complete pathological resection, complete response, and toxic effects.
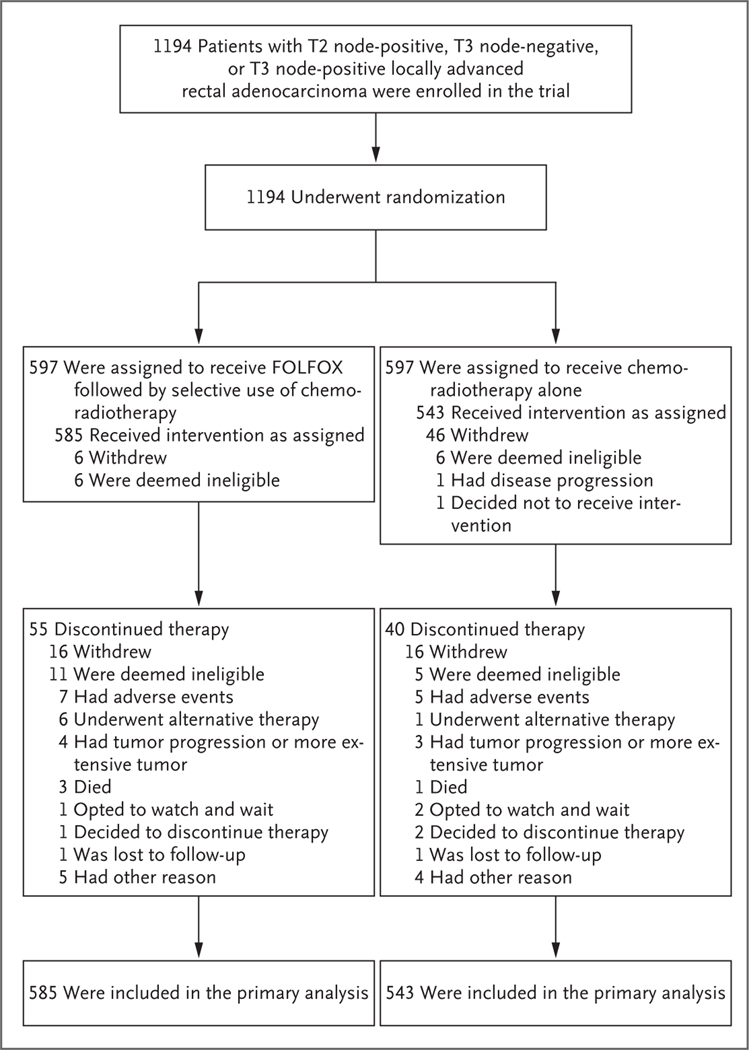
Results: From June 2012 through December 2018, a total of 1194 patients underwent randomization and 1128 started treatment; among those who started treatment, 585 were in the FOLFOX group and 543 in the chemoradiotherapy group. At a median follow-up of 58 months, FOLFOX was noninferior to chemoradiotherapy for disease-free survival (hazard ratio for disease recurrence or death, 0.92; 90.2% confidence interval [CI], 0.74 to 1.14; P = 0.005 for noninferiority). Five-year disease-free survival was 80.8% (95% CI, 77.9 to 83.7) in the FOLFOX group and 78.6% (95% CI, 75.4 to 81.8) in the chemoradiotherapy group. The groups were similar with respect to overall survival (hazard ratio for death, 1.04; 95% CI, 0.74 to 1.44) and local recurrence (hazard ratio, 1.18; 95% CI, 0.44 to 3.16). In the FOLFOX group, 53 patients (9.1%) received preoperative chemoradiotherapy and 8 (1.4%) received postoperative chemoradiotherapy.
Conclusions: In patients with locally advanced rectal cancer who were eligible for sphincter-sparing surgery, preoperative FOLFOX was noninferior to preoperative chemoradiotherapy with respect to disease-free survival. (Funded by the National Cancer Institute; PROSPECT ClinicalTrials.gov number, NCT01515787.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Preoperative Treatment of Locally Advanced Rectal Cancer.N Engl J Med. 2023 Oct 26;389(17):1630-1631. doi: 10.1056/NEJMc2309857. N Engl J Med. 2023. PMID: 37888928 No abstract available.
-
Preoperative Treatment of Locally Advanced Rectal Cancer.N Engl J Med. 2023 Oct 26;389(17):1631. doi: 10.1056/NEJMc2309857. N Engl J Med. 2023. PMID: 37888929 No abstract available.
-
Preoperative Treatment of Locally Advanced Rectal Cancer. Reply.N Engl J Med. 2023 Oct 26;389(17):1631-1632. doi: 10.1056/NEJMc2309857. N Engl J Med. 2023. PMID: 37888930 No abstract available.
-
Optimising local treatment decisions for rectal cancer.Lancet Gastroenterol Hepatol. 2024 Sep;9(9):779-781. doi: 10.1016/S2468-1253(24)00191-2. Lancet Gastroenterol Hepatol. 2024. PMID: 39127067 No abstract available.
References
-
- NIH consensus conference: adjuvant therapy for patients with colon and rectal cancer. JAMA 1990; 264:1 444–50. - PubMed
-
- Chau I, Brown G, Cunningham D, et al. Neoadjuvant capecitabine and oxaliplatin followed by synchronous chemoradiation and total mesorectal excision in magnetic resonance imaging-defined poor-risk rectal cancer. J Clin Oncol 2006; 24:6 68–74. - PubMed
-
- Douglass HO Jr, Moertel CG, Mayer RJ, et al. Survival after postoperative combination treatment of rectal cancer. N Engl J Med 1986; 315:1 294–5. - PubMed
-
- Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 1991; 324:7 09–15. - PubMed
-
- Peeters KCMJ Marijnen CAM, Nagtegaal ID, et al. The TME trial after a median follow-up of 6 years: increased local control but no survival benefit in irradiated patients with resectable rectal carcinoma. Ann Surg 2007; 246: 693–701. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- UG1 CA233290/CA/NCI NIH HHS/United States
- UG1 CA233329/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- UG1 CA233373/CA/NCI NIH HHS/United States
- UG1 CA189823/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- P30 CA006516/CA/NCI NIH HHS/United States
- UM1 CA233080/CA/NCI NIH HHS/United States
- K05 CA169384/CA/NCI NIH HHS/United States
- UG1 CA232760/CA/NCI NIH HHS/United States
- R01 CA131847/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical