

Intrahepatic Glissonean Approach for Robotic Anatomical Liver Resection of Segment 7 Using the Saline-Linked Monopolar Cautery Scissors (SLiC-Scissors) Method: A Technical Case Report With Videos
- PMID: 37273316
- PMCID: PMC10236908
- DOI: 10.7759/cureus.38470
Intrahepatic Glissonean Approach for Robotic Anatomical Liver Resection of Segment 7 Using the Saline-Linked Monopolar Cautery Scissors (SLiC-Scissors) Method: A Technical Case Report With Videos
Abstract
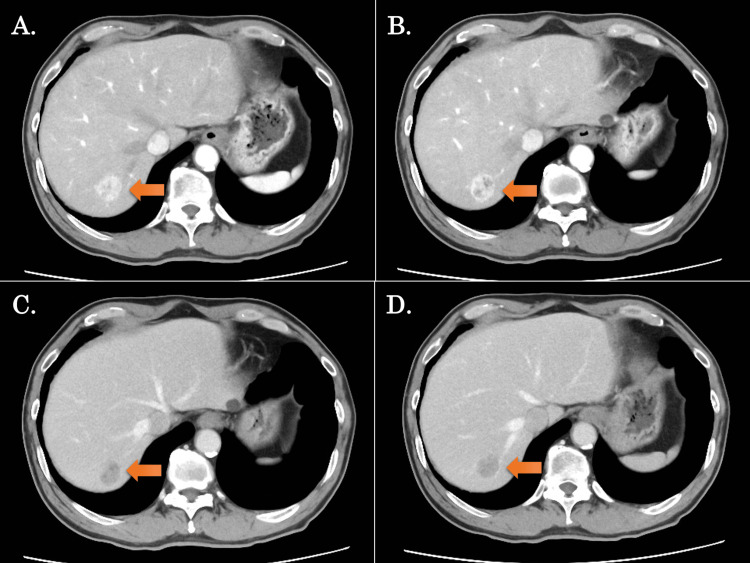
Anatomical hepatectomy of segment 7 (S7) is technically difficult due to its difficult accessibility. Here, we present our experience of robotic anatomical S7 subsectionectomy of the liver employing the saline-linked cautery scissors (SLiC-Scissors) technique. After the right lobe was fully mobilized, dissection of the Glissonean pedicle and hepatic venous branch of S7, as well as the liver parenchymal transection, were safely performed using the SLiC-Scissors method. Despite its technological complexity, the intrahepatic Glissonean approach for robotic anatomical S7 subsectionectomy of the liver employing the SLiC scissors method is safe and efficient.
Keywords: anatomical s7 subsectionectomy; hepatocellular carcinoma; liver parenchymal transection; robotic liver resection; saline-linked cautery scissors.
Copyright © 2023, Fujikawa et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Intrahepatic Glissonean pedicle approach to segment 7 from the dorsal side during laparoscopic anatomic hepatectomy of the cranial part of the right liver. Okuda Y, Honda G, Kobayashi S, Sakamoto K, Homma Y, Honjo M, Doi M. J Am Coll Surg. 2018;226:0–6. - PubMed
-
- Laparoscopic liver resection using the lateral approach from intercostal ports in segments VI, VII, and VIII. Inoue Y, Suzuki Y, Fujii K, et al. J Gastrointest Surg. 2017;21:2135–2143. - PubMed
-
- A standardized technique for right segmental liver resections. Machado MA, Herman P, Machado MC. Arch Surg. 2003;138:918–920. - PubMed
-
- Laparoscopic liver resection for segment VII lesion using a combination of rubber band retraction method and flexible laparoscope. Lee JW, Choi SH, Kim S, Kwon SW. Surg Endosc. 2020;34:954–960. - PubMed
LinkOut - more resources
Full Text Sources