

Secondary Mitral Regurgitation: Cardiac Remodeling, Diagnosis, and Management
- PMID: 37273859
- PMCID: PMC10236886
- DOI: 10.1016/j.shj.2022.100129
Secondary Mitral Regurgitation: Cardiac Remodeling, Diagnosis, and Management
Abstract
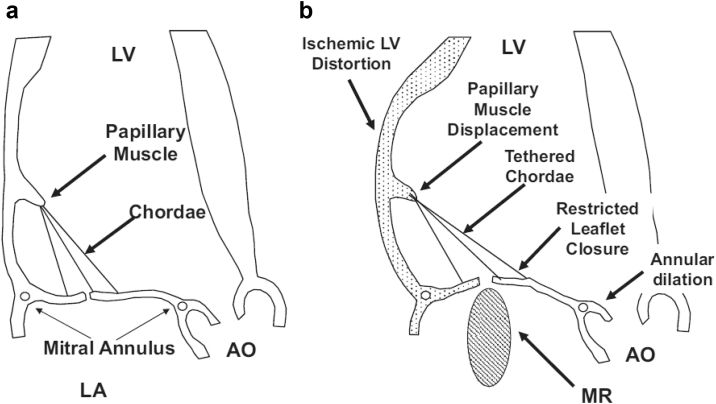
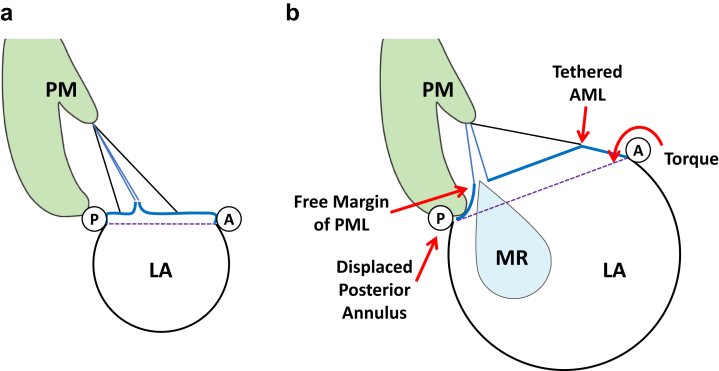
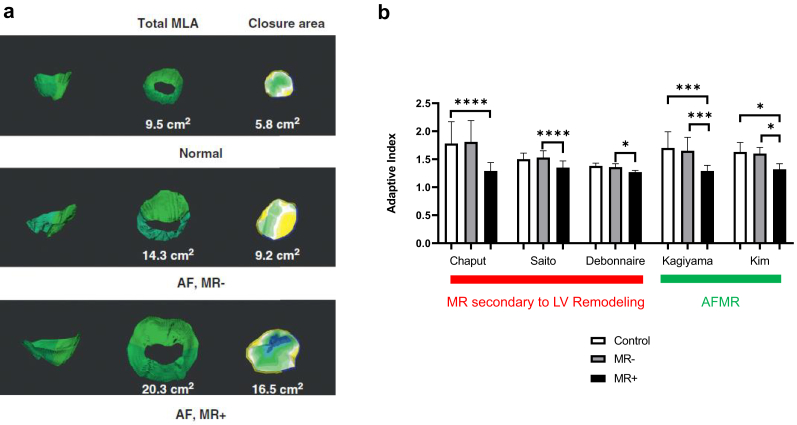
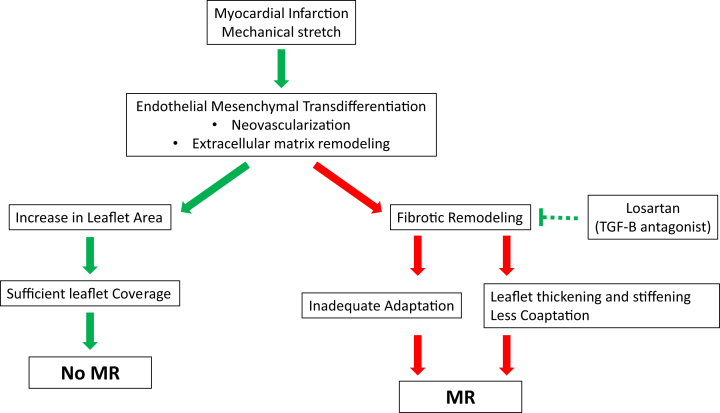
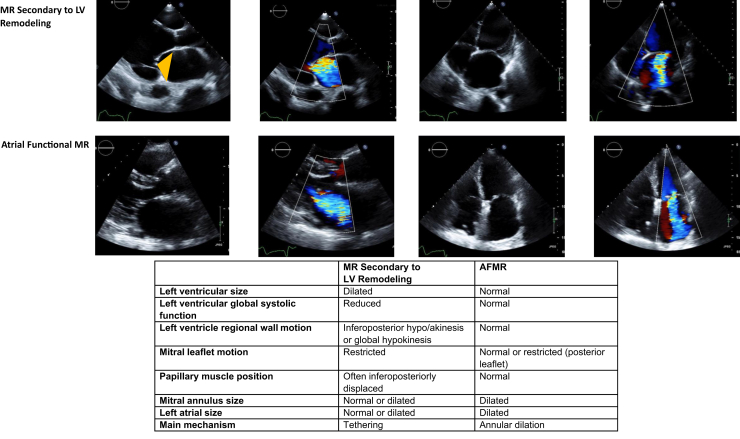
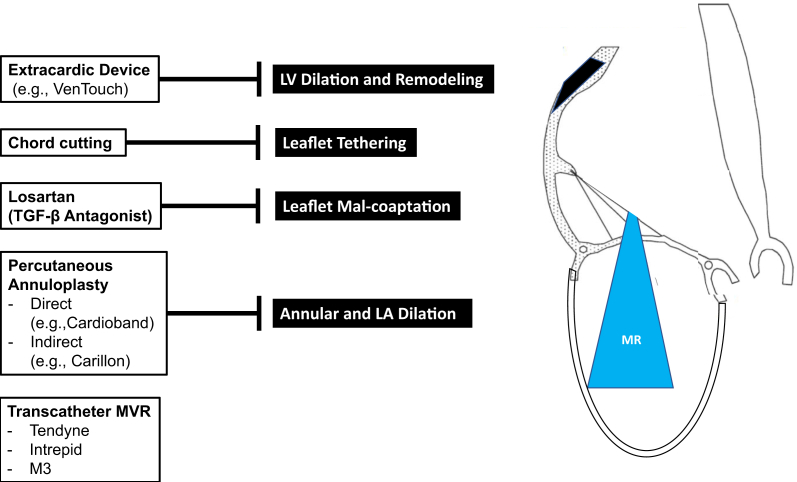
Secondary mitral regurgitation (MR) refers to MR resulting from left ventricular or left atrial remodeling. In ischemic or nonischemic cardiomyopathy, left ventricular dilation (regional or global) leads to papillary muscle displacement, tethering, and leaflet malcoaptation. In atrial functional MR, MR occurs in patients with left atrial dilation and altered mitral annular geometry due to atrial fibrillation. In addition to cardiac remodeling, leaflet remodeling is increasingly recognized. Mitral leaflet tissue actively adapts through leaflet growth to ensure adequate coaptation. Leaflets, however, can also undergo maladaptive thickening and fibrosis, leading to increased stiffness. The balance of cardiac and leaflet remodeling is a key determinant in the development of secondary MR. Clinical management starts with detection, severity grading, and identification of the underlying mechanism, which relies heavily on echocardiography. Treatment of secondary MR consists of guideline-directed medical therapy, surgical repair or replacement, and transcatheter edge-to-edge repair. Based on a better understanding of pathophysiology, novel percutaneous mitral repair and replacement devices have been developed and clinical trials are underway.
Keywords: Echocardiography; Heart failure; Mitral regurgitation.
© 2022 The Authors.
Figures


References
-
- Nkomo V.T., Gardin J.M., Skelton T.N., Gottdiener J.S., Scott C.G., Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Dziadzko V., Dziadzko M., Medina-Inojosa J.R., et al. Causes and mechanisms of isolated mitral regurgitation in the community: clinical context and outcome. Eur Heart J. 2019;40:2194–2202. - PubMed
-
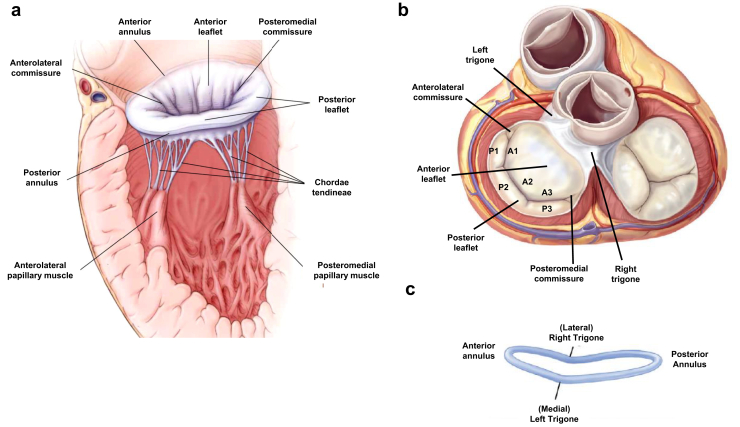
- McCarthy K.P., Ring L., Rana B.S. Anatomy of the mitral valve: understanding the mitral valve complex in mitral regurgitation. Eur J Echocardiogr. 2010;11:i3–i9. - PubMed
-
- Muresian H. The clinical anatomy of the mitral valve. Clin Anat. 2009;22:85–98. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
