

The emerging role of sacubitril/valsartan in pulmonary hypertension with heart failure
- PMID: 37273885
- PMCID: PMC10233066
- DOI: 10.3389/fcvm.2023.1125014
The emerging role of sacubitril/valsartan in pulmonary hypertension with heart failure
Abstract
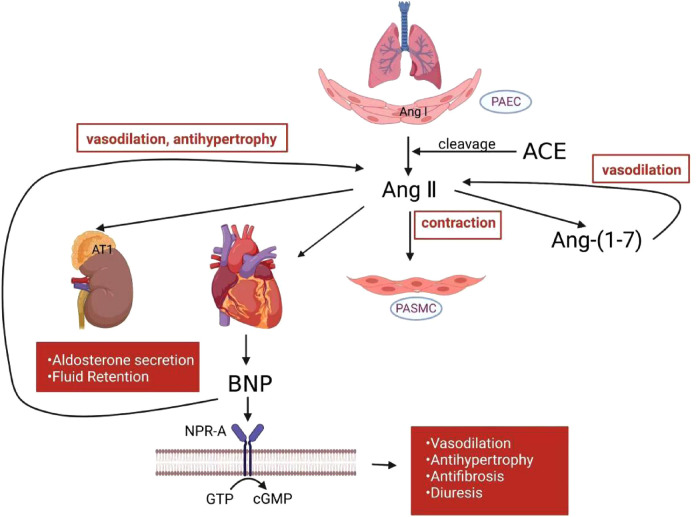
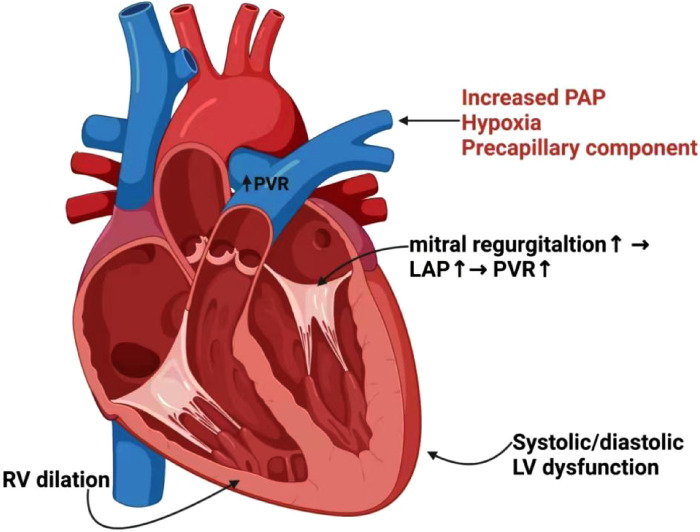
Pulmonary hypertension due to left heart disease (PH-LHD) represents approximately 65%-80% of all patients with PH. The progression, prognosis, and mortality of individuals with left heart failure (LHF) are significantly influenced by PH and right ventricular (RV) dysfunction. Consequently, cardiologists should devote ample attention to the interplay between HF and PH. Patients with PH and HF may not receive optimal benefits from the therapeutic effects of prostaglandins, endothelin receptor antagonists, or phosphodiesterase inhibitors, which are specific drugs for pulmonary arterial hypertension (PAH). Sacubitril/valsartan, the angiotensin receptor II blocker-neprilysin inhibitor (ARNI), was recommended as the first-line therapy for patients with heart failure with reduced ejection fraction (HFrEF) by the 2021 European Society of Cardiology Guidelines. Although ARNI is effective in treating left ventricular (LV) enlargement and lower ejection fraction, its efficacy in treating individuals with PH and HF remains underexplored. Considering its vasodilatory effect at the pre-capillary level and a natriuretic drainage role at the post-capillary level, ARNI is believed to have a broad range of potential applications in treating PH-LHD. This review discusses the fundamental pathophysiological connections between PH and HF, emphasizing the latest research and potential benefits of ARNI in PH with various types of LHF and RV dysfunction.
Keywords: clinical benefits; left heart failure; pharmacological mechanism; pulmonary hypertension; right ventricular dysfunction; sacubitril/valsartan.
© 2023 Xu, Yang, Hui, Zhang, Bian, Tao, Lu, Wang, Qian and Shang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Neprilysin Inhibitors in Heart Failure: The Science, Mechanism of Action, Clinical Studies, and Unanswered Questions.JACC Basic Transl Sci. 2022 Sep 7;8(1):88-105. doi: 10.1016/j.jacbts.2022.05.010. eCollection 2023 Jan. JACC Basic Transl Sci. 2022. PMID: 36777165 Free PMC article. Review.
-
Reduction in pulmonary artery pressures with use of sacubitril/valsartan.J Cardiol Cases. 2019 Aug 23;20(5):187-190. doi: 10.1016/j.jccase.2019.08.006. eCollection 2019 Nov. J Cardiol Cases. 2019. PMID: 31719942 Free PMC article.
-
Sacubitril/valsartan affects pulmonary arterial pressure in heart failure with preserved ejection fraction and pulmonary hypertension.ESC Heart Fail. 2022 Aug;9(4):2170-2180. doi: 10.1002/ehf2.13952. Epub 2022 May 19. ESC Heart Fail. 2022. PMID: 35588235 Free PMC article.
-
Impact of sacubitril/valsartan on echo parameters in heart failure patients with reduced ejection fraction a prospective evaluation.Int J Cardiol Heart Vasc. 2019 Sep 3;25:100418. doi: 10.1016/j.ijcha.2019.100418. eCollection 2019 Dec. Int J Cardiol Heart Vasc. 2019. PMID: 31517034 Free PMC article.
-
Angiotensin Receptor Neprilysin Inhibition in Heart Failure With Preserved Ejection Fraction: Rationale and Design of the PARAGON-HF Trial.JACC Heart Fail. 2017 Jul;5(7):471-482. doi: 10.1016/j.jchf.2017.04.013. Epub 2017 Jun 26. JACC Heart Fail. 2017. PMID: 28662936 Review.
Cited by
-
Empagliflozin combined with sacubitril/valsartan in hypertensive patients with heart failure: a retrospective study of efficacy and effect on blood pressure variability and cardiac function.Am J Transl Res. 2024 Jul 15;16(7):3036-3045. doi: 10.62347/LXJB8350. eCollection 2024. Am J Transl Res. 2024. PMID: 39114702 Free PMC article.
References
-
- Guazzi M, Dixon D, Labate V, Beussink-Nelson L, Bandera F, Cuttica MJ, et al. RV contractile function and its coupling to pulmonary circulation in heart failure with preserved ejection fraction: stratification of clinical phenotypes and outcomes. JACC Cardiovasc Imaging. (2017) 10(10 Pt B):1211–21. 10.1016/j.jcmg.2016.12.024 - DOI - PubMed
-
- Maron BA, Leopold JA. Emerging concepts in the molecular basis of pulmonary arterial hypertension: part II: neurohormonal signaling contributes to the pulmonary vascular and right ventricular pathophenotype of pulmonary arterial hypertension. Circulation. (2015) 131(23):2079–91. 10.1161/CIRCULATIONAHA.114.006980 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous