

Comparison of long-term quality of life based on surgical procedure in patients with rectal cancer
- PMID: 37274255
- PMCID: PMC10235785
- DOI: 10.3389/fonc.2023.1197131
Comparison of long-term quality of life based on surgical procedure in patients with rectal cancer
Abstract
Introduction: Reports on the long-term quality of life (QOL) over 3 years after surgery in patients who have undergone surgery for rectal cancer are limited. Therefore, we aimed to evaluate the long-term QOL of patients who underwent high anterior resection (HAR), low anterior resection (LAR), internal sphincter resection (ISR), or abdominoperineal resection (APR) for rectal cancer.
Methods: A questionnaire regarding QOL was sent to 360 patients with rectal cancer who underwent curative resection by HAR, LAR, ISR, or APR between January 2005 and December 2015. QOL was assessed using the short-form 36 (SF-36) and modified fecal incontinence QOL (mFIQL) questionnaire. QOL between surgical procedures was analyzed using a multivariate model adjusted for age, sex, and postoperative time.
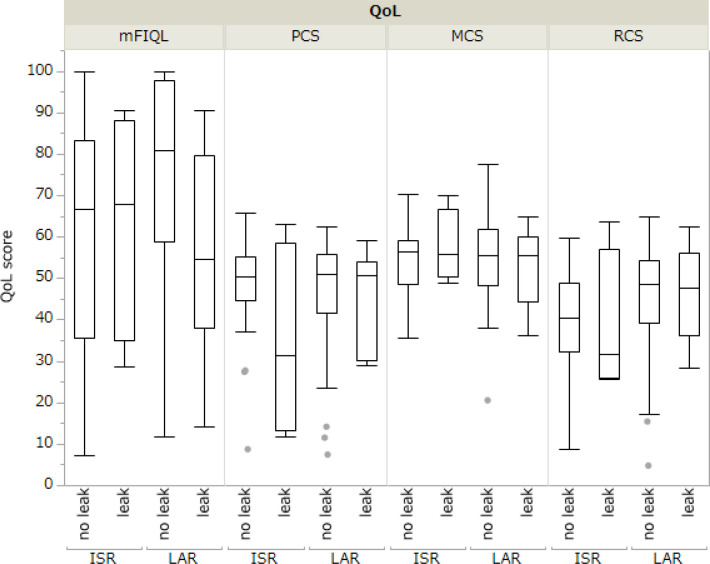
Results: A total of 144 patients responded with a median follow-up period of 94 months (range 38-233 months). According to surgical procedure, HAR was performed in 26 patients, LAR in 80 patients, ISR in 32 patients, and APR in 6 patients. Patients who underwent HAR had significantly better mFIQL scores than those who underwent LAR and ISR (p=0.013 and p=0004, respectively) and significantly better role/social component summary scores on the SF-36 subscales (p=0.007). No difference was observed in the mFIQL scores between patients who underwent ISR and those who underwent APR (p=0.8423). In addition, postoperative anastomotic leakage sutures did not influence the mFIQL and SF-36 scores after surgery.
Conclusion: The QOL of patients who underwent anus-preserving surgery was best in the HAR group, with the QOL of other groups similar to the APR group. These results suggest that anus- preserving surgery is acceptable from a QOL standpoint. However, a colostomy may be a more satisfactory procedure in some patients.
Keywords: anus-preserving; high anterior resection; internal sphincter; long-term; low anterior resection; quality of life; rectal cancer; surgery.
Copyright © 2023 Yuge, Miwa, Fujita, Murotani, Shigaki, Yoshida, Yoshida, Koushi, Fujiyoshi, Nagasu and Akagi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous