

Varied Clinical Presentations of Allergic Fungal Rhinosinusitis-A Case Series
- PMID: 37275020
- PMCID: PMC10234982
- DOI: 10.1007/s12070-022-03338-0
Varied Clinical Presentations of Allergic Fungal Rhinosinusitis-A Case Series
Abstract
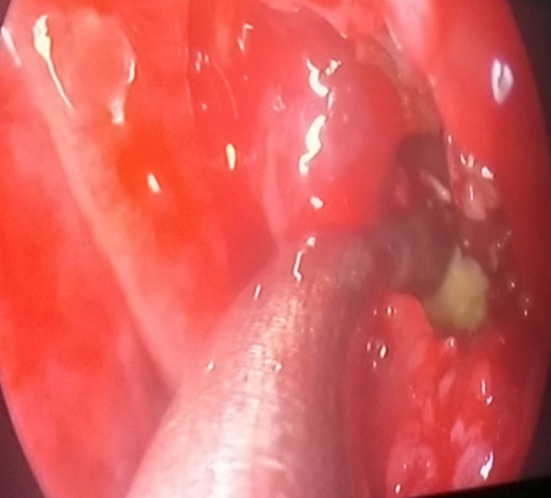
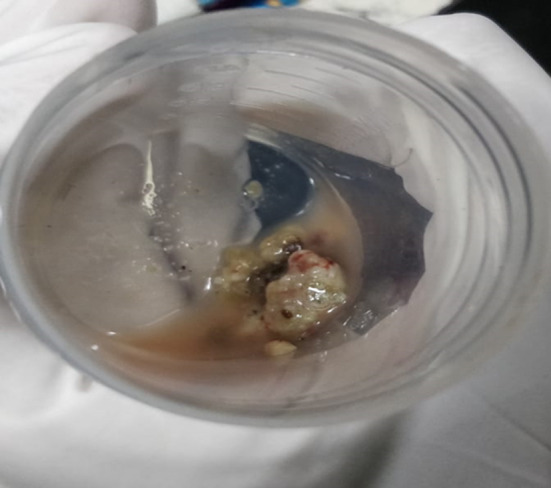
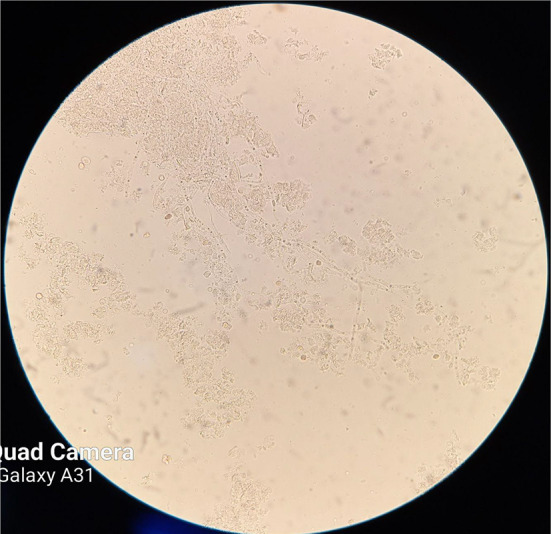
Fungal sinusitis is broadly classified into invasive and non invasive types. Invasive type presents with fungal hyphae within the mucosa, submucosa, bone, or blood vessels of the paranasal sinuses and includes Acute Invasive Fungal Sinusitis, Acute Fulminant, Chronic Invasive Fungal Sinusitis, Chronic Granulomatous Fungal Sinusitis. Invasive forms of fungal rhinosinusitis are rare and confined to groups of patients who are immunocompromised (Key in Fungal rhinosinusitis). Noninvasive type shows absence of fungal hyphae within the mucosa paranasal sinuses. It includes Allergic Fungal rhinosinusitis, Fungus Ball (fungus mycetoma). The study was performed on a total of 30 patients, in Department of Otorhinolaryngology, at our hospital after getting approved by the Instituitional Human Ethical Committee. We selected 30 patients diagnosed with allergic fungal sinusitis and studied their varied clinical presentations and treatment for a period of 1 year. It was a prospective case series type of study. Patients who presented with symptoms of allergic fungal rhinosinusitis were included. Patients who were referred with complaints of proptosis, diplopia were also included to rule out allergic fungal rhinosinusitis and its complications. Patients diagnosed with chronic granulomatous infection of nose and invasive fungal sinusitis were excluded. Evaluation of patients involved a detailed case history followed by clinical examination and radiologic investigation. After getting proper consent, we did a study of 30 patients who presented to our outpatient department with complaints of sinusitis. Our study included 12 male and 18 female patients. Among these patients, all of them had complaints of frequent allergic rhinosinusitis, nose block, facial heaviness. 12 among them had olfactory disturbances, reduced perception of smell. 4 patients presented with visual disturbances and proptosis which subsided after endoscopic sinus surgery was done.24 among these patients had presence of allergic fungal mucin in their nasal secretions and 10 patients had history of associated atopy and asthma and elevated Ig E levels. And 20 of these patients showed high eosinophil counts. All these patients in our case series were under the age group 22-70 years. These patients were treated with a course of nasal sprays and preoperative steroids in case of extensive polyposis and were taken up for functional endoscopic sinus surgery. Polypoidal mucosa was removed, diseased tissue was cleared, sinus blockage was released and fungal mucin/tissue bits were sent for histopathological analysis, KOH mount and fungal culture. This study included a series of cases which showed a wide range of the various clinical presentations that occur in cases of allergic fungal rhinosinusitis, its diagnosis and treatment. The advantage of this study was we had analyzed a good number of cases with varied presentations. Since AFRS is closely related with EMRS, CRS a proper clinical, radiological and immunological evaluation of the cases help in knowing the correct diagnosis and treatment.
Keywords: Allergy; Fungal culture; Mucin; Polyps; Sinusitis.
© Association of Otolaryngologists of India 2022. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of interestThere is no conflict of interest.
Figures














References
-
- Mulhem NA, Al Momen A, Almolani F. The different clinical presentations of allergic fungal rhinosinusitis. Otolaryngol Open Access J. 2018;3(2):000172. doi: 10.23880/OOAJ-16000172. - DOI
-
- Göde S, Karcı B, Woessner K. All around the nose. Cham: Springer; 2020. Allergic fungal rhinosinusitis; pp. 235–237.
LinkOut - more resources
Full Text Sources