

A Fondazione Italiana Linfomi cohort study of R-COMP vs R-CHOP in older patients with diffuse large B-cell lymphoma
- PMID: 37276080
- PMCID: PMC10407138
- DOI: 10.1182/bloodadvances.2023009839
A Fondazione Italiana Linfomi cohort study of R-COMP vs R-CHOP in older patients with diffuse large B-cell lymphoma
Abstract
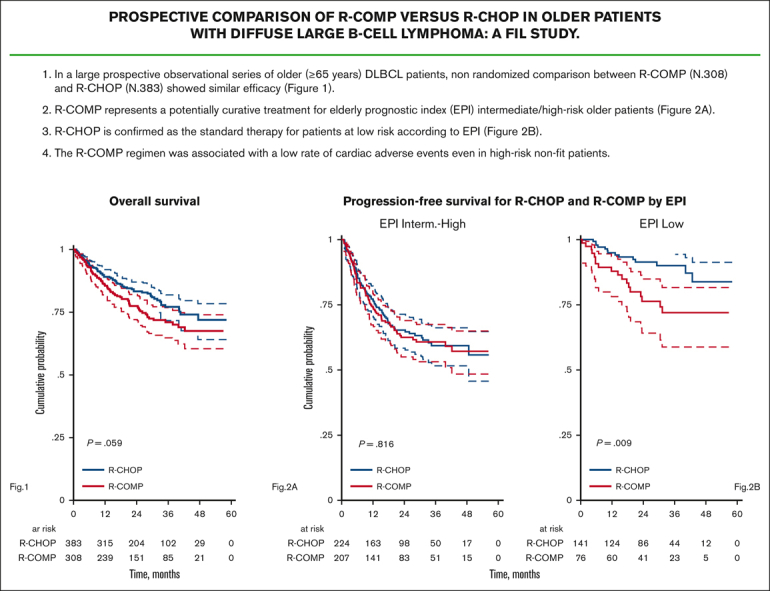
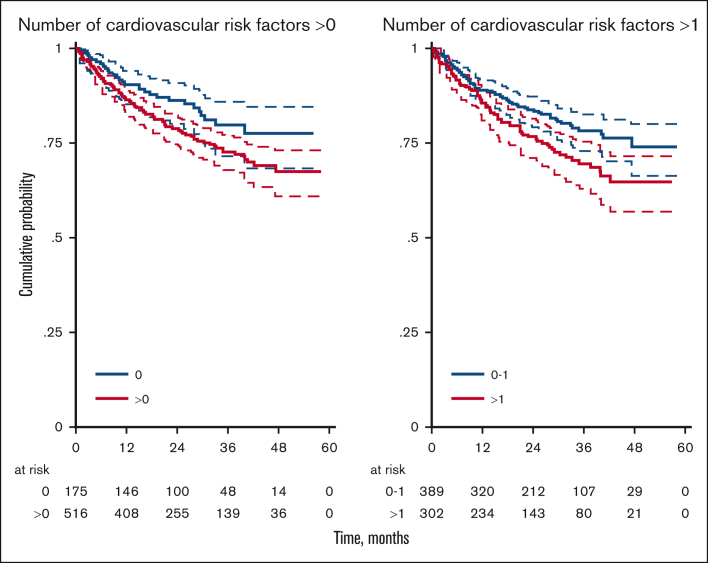
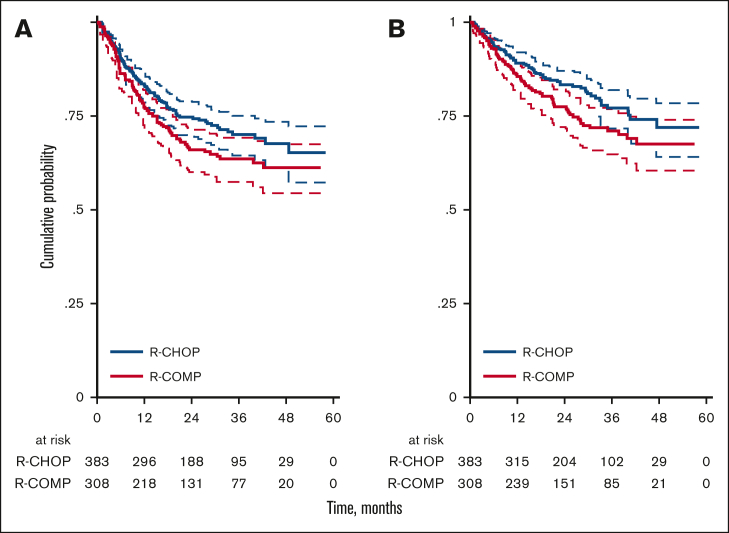
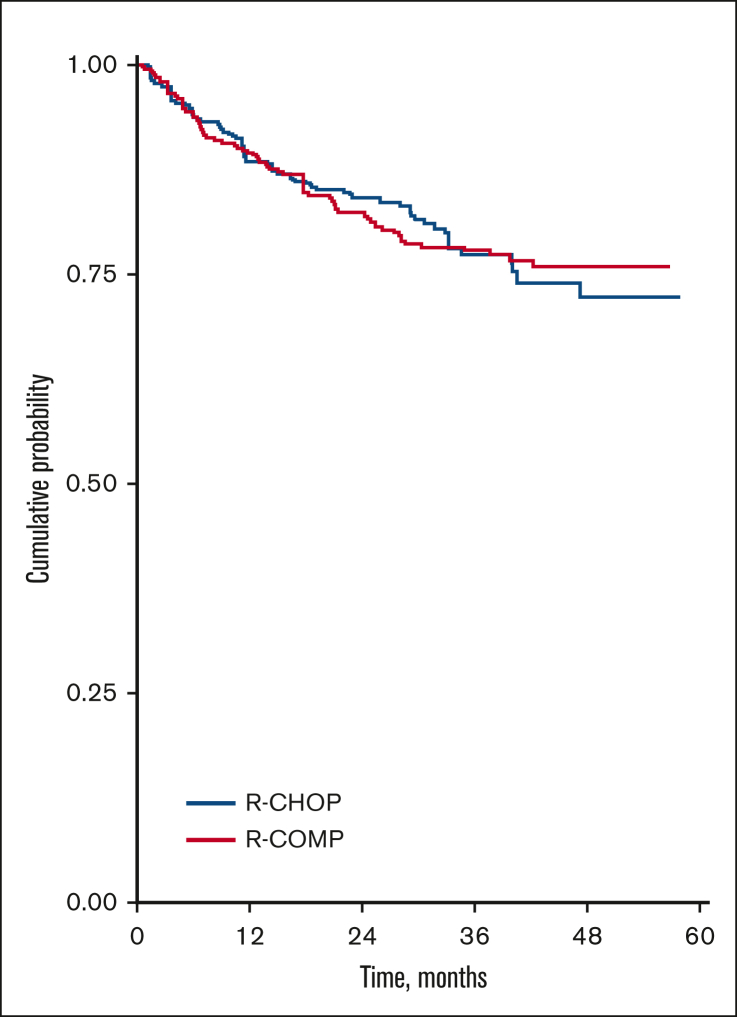
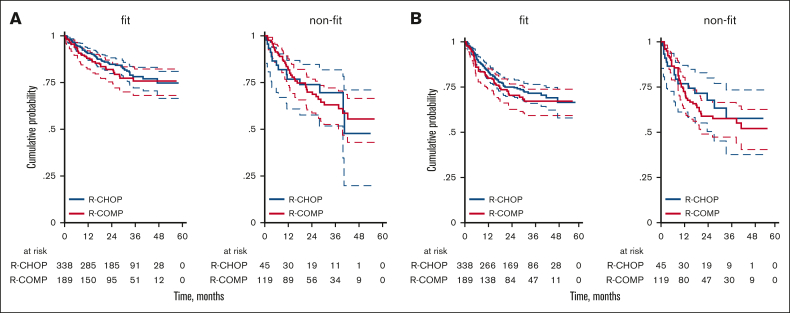
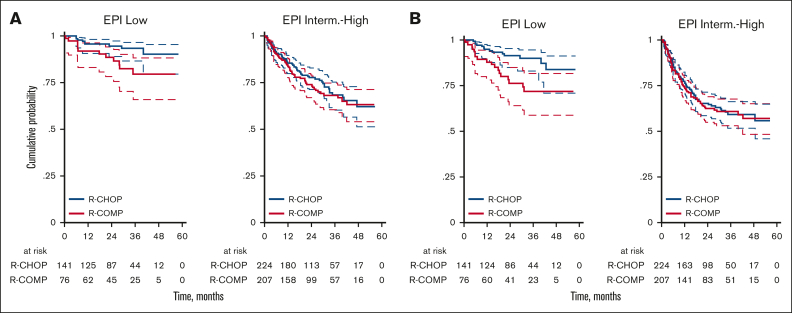
Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is the most commonly used regimen for the upfront treatment of diffuse large B-cell lymphoma (DLBCL). However, it is associated with cardiotoxicity, especially in older patients. Substituting doxorubicin with non-PEGylated liposomal doxorubicin (R-COMP) may reduce the risk of cardiac events, but its efficacy has never been demonstrated in prospective trials. We describe the characteristics and outcome of patients with DLBCL aged ≥65 years prospectively enrolled in the Elderly Project by the Fondazione Italiana Linfomi and treated with full doses of R-CHOP or R-COMP per local practice. Starting from 1163 patients, 383 (55%) were treated with R-CHOP and 308 (45%) with R-COMP. Patients treated with R-COMP were older (median age, 76 vs 71 years), less frequently fit at simplified geriatric assessment (61% vs 88%; P < .001), and had a more frequent baseline cardiac disorders (grade >1, 32% vs 8%; P < .001). Three-year progression-free survival (PFS) was similar between R-CHOP and R-COMP (70% and 64%); 3-year overall survival was 77%, and 71% respectively. R-CHOP was associated with better PFS vs R-COMP only in the Elderly Prognostic Index (EPI) low-risk group. The two groups had similar rates of treatment interruptions due to toxicities or of cardiac events (P = 1.00). We suggest R-COMP is a potentially curative treatment for older patients with intermediate- or high-risk EPI, even in the presence of a baseline cardiopathy. R-CHOP is confirmed as the standard therapy for low risk patients.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: A.A. is a member of advisory board for Novartis, Janssen, and AbbVie. A.T. receives honoraria directly received from an entity: Takeda, Kiowa Kyrin, and MSD, and is a member of advisory board for Janssen, Gentili, and Sanofi. F.C. provides consultancy within the past 2 years for AstraZeneca and Roche; receives research funding from Roche; and is a member of advisory board for Roche. A.F. is a member of advisory board for Roche, Janssen, Takeda, Kyowa Kirin, Servier, Incyte, and Gilead. M.B. is a member of advisory board for Roche, Takeda, Kiowa, Gilead, Novartis, Incyte, and Janssen; reports research funding from Roche; and reports membership on another entity's board of directors or its advisory committees for Fondazione Italiana Linfomi (nonprofit foundation). S.L. provides consultancy within the past 2 years for GenMAb, Regeneron, Incyte, Takeda, and is a member of advisory board for Roche, Bristol Myers Squibb (BMS), GenMAb, Janssen, Kite, Gilead, and Regeneron. V.R.Z. receives honoraria from Janssen and is a member of advisory board for Gilead and Novartis. G.M. provides consultancy within the past 2 years for Janssen, Incite, Roche, and AbbVie; received honoraria directly from an entity: Janssen, Incyte, Roche, and AbbVie, and is a member of advisory board for Janssen, Incyte, Roche, and AbbVie. G.G. is a member of advisory board for Roche, Celgene/BMS, Kite/Gilead, Janssen, Takeda, and Servier. S.H. provides consultancy within the past 2 years with Incyte, Ipsen, MSD, Gilead, Novartis, Roche, and Takeda, and receives research funding from Ministero Dell'Istruzione e del Merito (PRIN 2017PPS2X4). M.T. has provided consultancy within the past 2 years for Incyte and is a member of advisory board for Incyte, BeiGene, AbbVie, and Kiowa-Kirin. L.N. provides consultancy for Takeda, Incyte, Kyowa Kirin, Roche, and Janssen. S.F. has provided consultancy within the past 2 years for EusaPharma, Janssen, Sandoz, and AbbVie; receives research funding from Janssen, MorphoSys, and Gilead; receives honoraria directly from an entity: Janssen, EusaPharma, Servier, and Gentili; and is a member of advisory board for EusaPharma, Janssen, Clinigen, Incyte, and Italfarmaco. L.M. has been a scientific consultant within the past 2 years for Sandoz (free of fee). V.T. has provided consultancy within the past 2 years for Sandoz (nonfinancial). M.S. receives honoraria directly from Gilead and Servier, and is a member of advisory board for Gilead, Servier, Novartis, Incyte, and BeiGene. F.M. is a member of the advisory board for Janssen, Gilead, MSD, Takeda, Roche, and Novartis, and has membership on the board of directors or its advisory committees in Fondazione Italiana Linfomi (nonprofit foundation). The remaining authors declare no competing financial interests.
Figures
References
-
- Coiffier B, Lepage E, Briere J, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;346(4):235–242. - PubMed
-
- Singal PK, Iliskovic N. Doxorubicin-induced cardiomyopathy. N Engl J Med. 1998;339(13):900–905. - PubMed
-
- Von Hoff DD, Layard MW, Basa P, et al. Risk factors for doxorubicin-induced congestive heart failure. Ann Intern Med. 1979;91(5):710–717. - PubMed
-
- Limat S, Demesmay K, Voillat L, et al. Early cardiotoxicity of the CHOP regimen in aggressive non-Hodgkin's lymphoma. Ann Oncol. 2003;14(2):277–281. - PubMed
-
- Wang L, Tan TC, Halpern EF, et al. Major cardiac events and the value of echocardiographic evaluation in patients receiving anthracycline-based chemotherapy. Am J Cardiol. 2015;116(3):442–446. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
