

Prevalence of and risk factors for microscopic and submicroscopic malaria infections in pregnancy: a systematic review and meta-analysis
- PMID: 37276878
- PMCID: PMC10880462
- DOI: 10.1016/S2214-109X(23)00194-8
Prevalence of and risk factors for microscopic and submicroscopic malaria infections in pregnancy: a systematic review and meta-analysis
Abstract
Background: Malaria infections during pregnancy can cause adverse birth outcomes, yet many infections are undetected by microscopy. We aimed to describe the epidemiology of submicroscopic malaria infections in pregnant women in Asia, the Americas, and Africa using aggregated and individual participant data (IPD).
Methods: For this systematic review and meta-analysis, studies (published Jan 1, 1997 to Nov 10, 2021) with information on both microscopic and submicroscopic infections during pregnancy from Asia, the Americas, or Africa, identified in the Malaria-in-Pregnancy Library, were eligible. Studies (or subgroups or study groups) that selected participants on the basis of the presence of fever or a positive blood smear were excluded to avoid selection bias. We obtained IPD (when available) and aggregated data. Estimates of malaria transmission intensity and sulfadoxine-pyrimethamine resistance, matched by study location and year, were obtained using publicly available data. One-stage multivariable logit and multinomial models with random intercepts for study site were used in meta-analysis to assess prevalence of and risk factors for submicroscopic infections during pregnancy and at delivery. This study is registered with PROSPERO, number CRD42015027342.
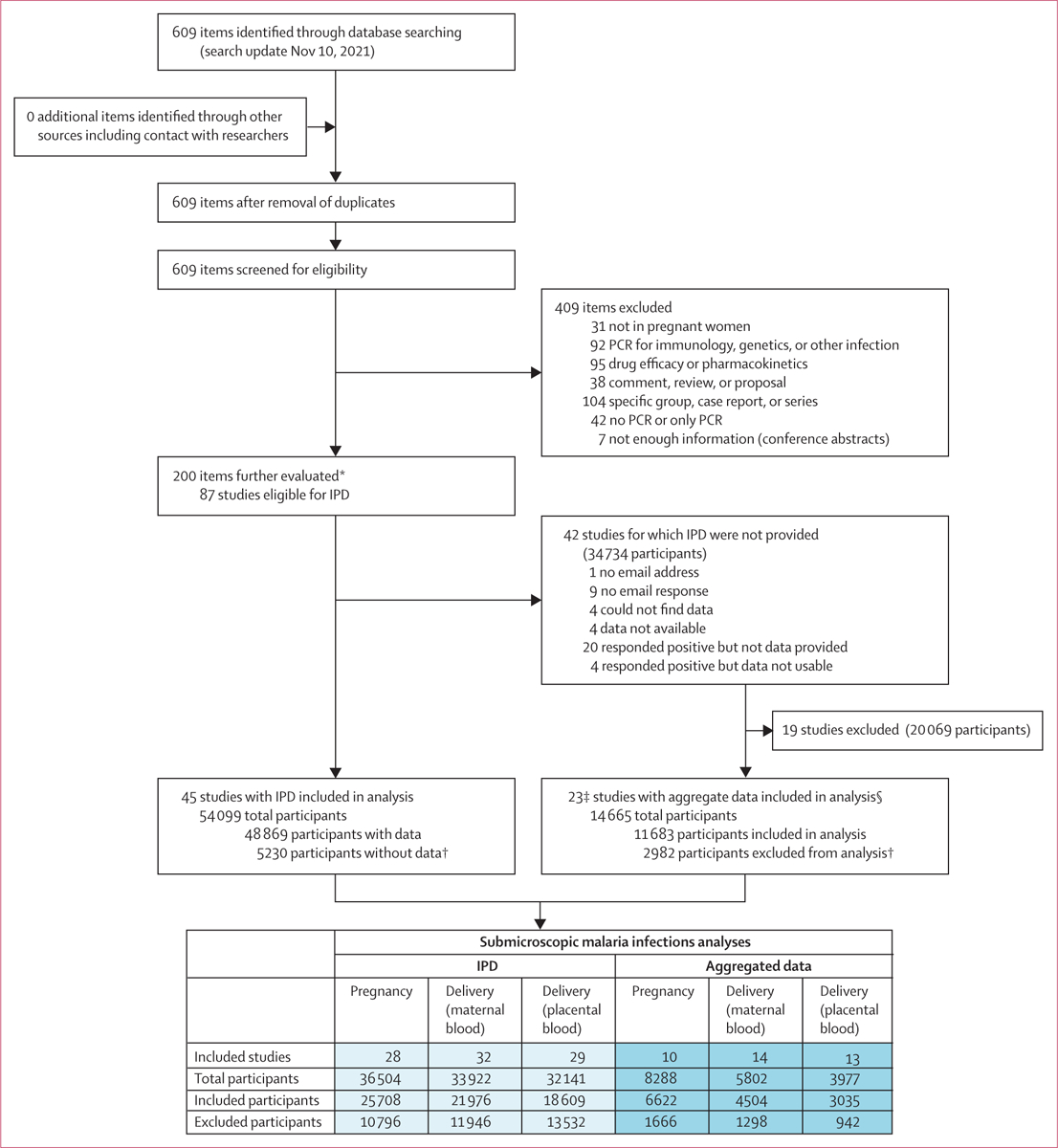
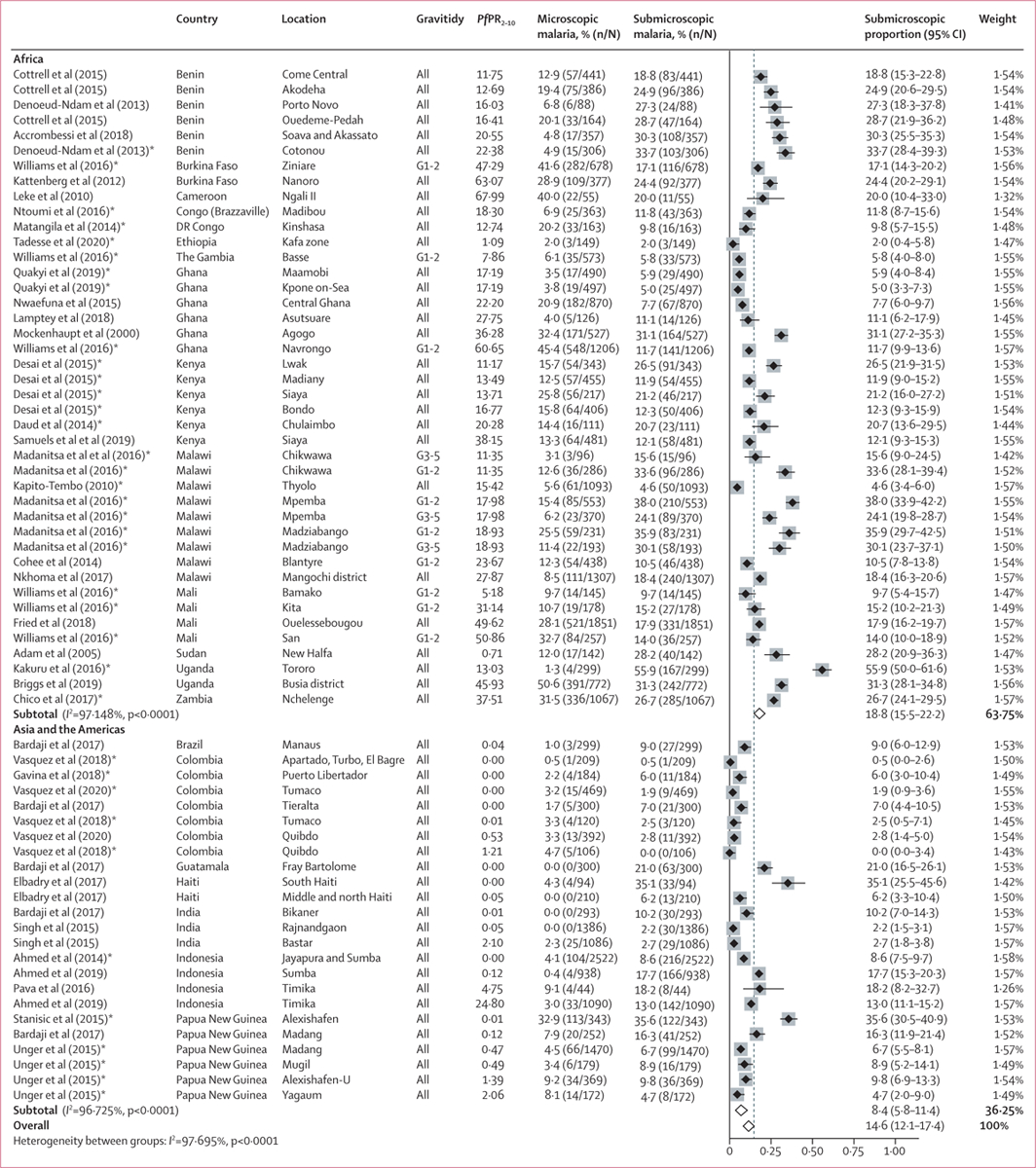
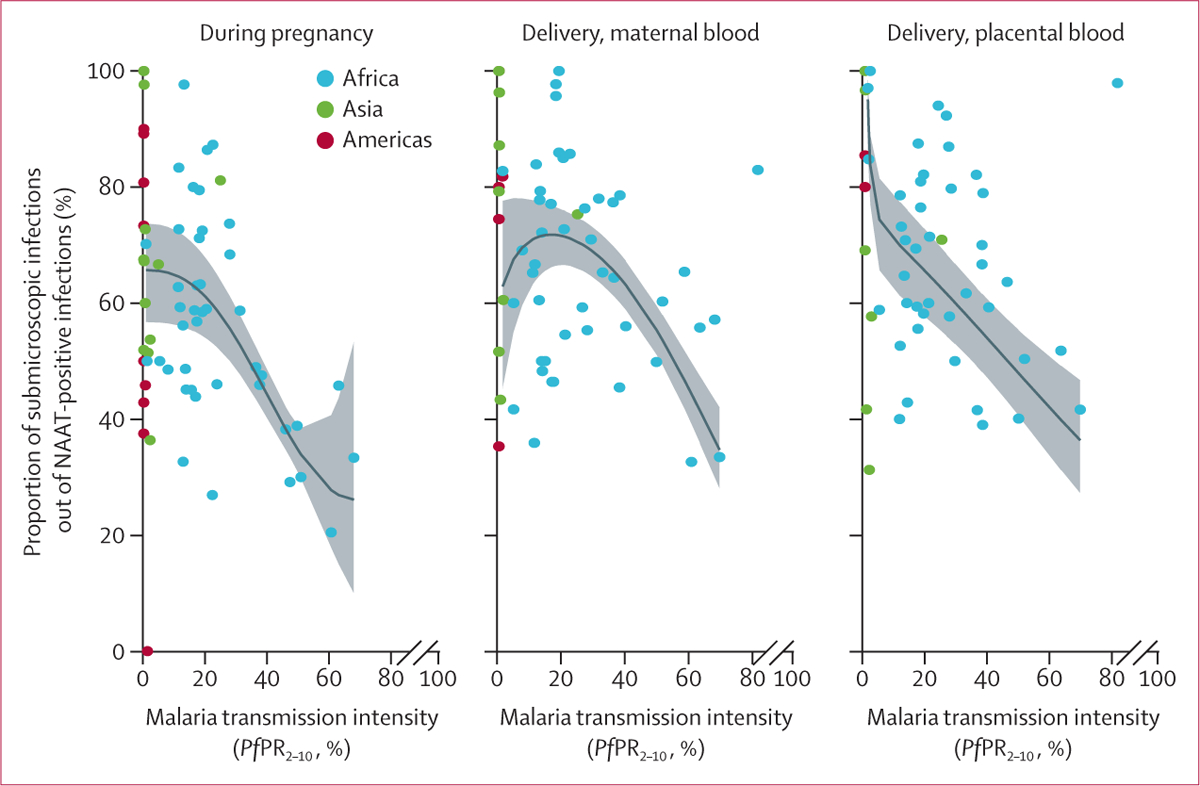
Findings: The search identified 87 eligible studies, 68 (78%) of which contributed to the analyses. Of these 68 studies, 45 (66%) studies contributed IPD (48 869 participants) and 23 (34%) studies contributed aggregated data (11 863 participants). During pregnancy, median prevalence estimates were 13·5% (range 0·0-55·9, 66 substudies) for submicroscopic and 8·0% (0·0-50·6, 66 substudies) for microscopic malaria. Among women with positive Plasmodium nucleic acid amplification tests (NAATs), the median proportion of submicroscopic infections was 58·7% (range 0·0-100); this proportion was highest in the Americas (73·3%, 0·0-100), followed by Asia (67·2%, 36·4-100) and Africa (56·5%, 20·5-97·7). In individual patient data analysis, compared with women with no malaria infections, those with submicroscopic infections were more likely to present with fever in Africa (adjusted odds ratio 1·32, 95% CI 1·02-1·72; p=0·038) but not in other regions. Among women with NAAT-positive infections in Asia and the Americas, Plasmodium vivax infections were more likely to be submicroscopic than Plasmodium falciparum infections (3·69, 2·45-5·54; p<0·0001). Risk factors for submicroscopic infections among women with NAAT-positive infections in Africa included older age (age ≥30 years), multigravidity, and no HIV infection.
Interpretation: During pregnancy, submicroscopic infections are more common than microscopic infections and are associated with fever in Africa. Malaria control in pregnancy should target both microscopic and submicroscopic infections.
Funding: Bill & Melinda Gates Foundation through the Worldwide Antimalarial Resistance Network.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
The silent threat of submicroscopic Plasmodium infections during pregnancy.Lancet Glob Health. 2023 Jul;11(7):e991-e992. doi: 10.1016/S2214-109X(23)00249-8. Epub 2023 Jun 2. Lancet Glob Health. 2023. PMID: 37276879 No abstract available.
References
-
- Rogerson SJ, Desai M, Mayor A, Sicuri E, Taylor SM, van Eijk AM. Burden, pathology, and costs of malaria in pregnancy: new developments for an old problem. Lancet Infect Dis 2018; 18: e107–18. - PubMed
-
- Moore KA, Simpson JA, Scoullar MJL, McGready R, Fowkes FJI. Quantification of the association between malaria in pregnancy and stillbirth: a systematic review and meta-analysis. Lancet Glob Health 2017; 5: e1101–12. - PubMed
-
- Rijken MJ, McGready R, Boel ME, et al. Malaria in pregnancy in the Asia-Pacific region. Lancet Infect Dis 2012; 12: 75–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
