

Meningiomas of the rolandic region: risk factors for motor deficit and role of intra-operative monitoring
- PMID: 37277557
- PMCID: PMC10319650
- DOI: 10.1007/s00701-023-05630-6
Meningiomas of the rolandic region: risk factors for motor deficit and role of intra-operative monitoring
Abstract
Objective: Meningiomas of the rolandic region are associated to high risk of postoperative motor deficits. This study discusses the factors affecting motor outcome and recurrences from the analysis of a monoinstitutional case series and eight studies from a literature review.
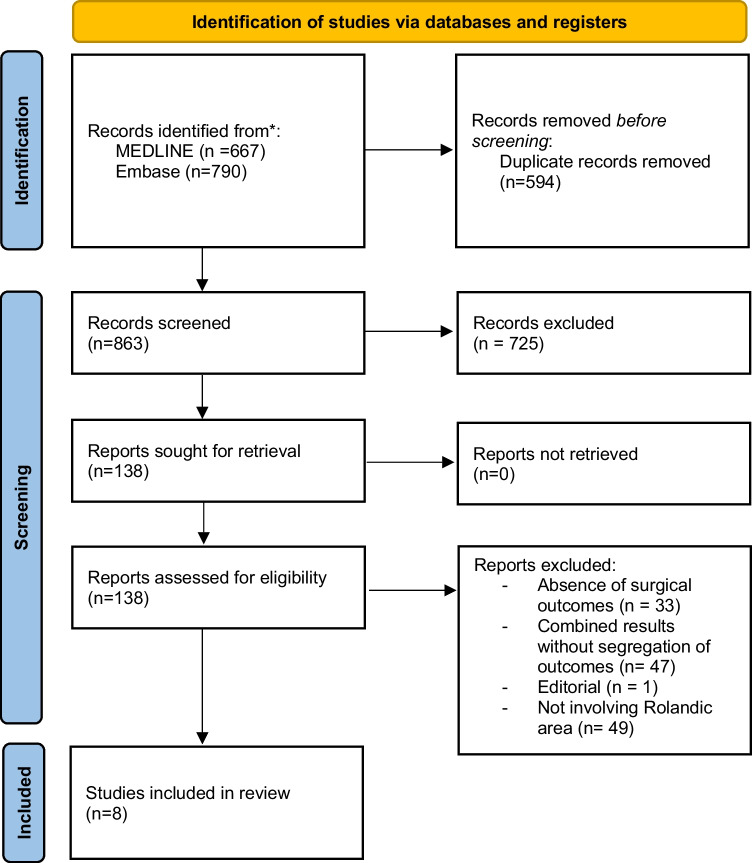
Methods: Data of 75 patients who underwent surgery for meningioma of the rolandic region were retrospectively reviewed. The analyzed factors included tumor location and size, clinical presentation, magnetic resonance imaging (MRI) and surgical findings, brain-tumor interface, extent of resection, postoperative outcome and recurrence. Eight studies from literature on rolandic meningiomas treated with or without intraoperative monitoring (IOM) were reviewed with the aim to define the impact of IOM on the extent of resection and motor outcome.
Results: Among the 75 patients of the personal series, the meningioma was on the brain convexity in 34 (46%), at the parasagittal region in 28 (37%) and at the falx in 13 (17%). The brain-tumor interface was preserved in 53 cases (71%) at MRI and in 56 (75%) at surgical exploration. Simpson grade I resection was obtained in 43% of patients, grade II in 33%, grade III in 15% and grade IV in 9%. The motor function worsened postoperatively in 9 among 32 cases with preoperative deficit (28%) and in 5 among 43 with no preoperative deficit (11.5%); definitive motor deficit was evidenced in overall series at follow-up in 7 (9.3%). Patients with meningioma with lost arachnoid interface had significant higher rates of worsened postoperative motor deficit (p = 0.01) and seizures (p = 0.033). Recurrence occurred in 8 patients (11%). The analysis of the 8 reviewed studies (4 with and 4 without IOM) shows in the group without IOM higher rates of Simpson grades I and II resection (p = 0.02) and lower rates of grades IV resection (p = 0.002); no significant differences in postoperative immediate and long-term motor deficits were evidenced between the two groups.
Conclusions: Data from literature review show that the use of IOM does not affect the postoperative motor deficit Therefore, its role in rolandic meningiomas resection remains to be determined and will be defined in further studies.
Keywords: Convexity; Falx; Intraoperative monitoring; Meningioma; Parasagittal; Rolandic region.
© 2023. The Author(s).
Conflict of interest statement
All authors deny any financial and not-financial competing interests.
Figures
Similar articles
-
Time to Recurrence of Intracranial Meningiomas from a Monoinstitutional Surgical Series.World Neurosurg. 2024 May;185:e612-e619. doi: 10.1016/j.wneu.2024.02.087. Epub 2024 Feb 28. World Neurosurg. 2024. PMID: 38417623
-
Predictors of postoperative motor function in rolandic meningiomas.J Neurosurg. 2018 May 25;130(4):1283-1288. doi: 10.3171/2017.12.JNS172423. Print 2019 Apr 1. J Neurosurg. 2018. PMID: 29799346
-
Rolandic area meningioma resection controlled and guided by intraoperative cortical mapping.Acta Neurochir (Wien). 2012 May;154(5):843-53. doi: 10.1007/s00701-012-1279-3. Epub 2012 Mar 17. Acta Neurochir (Wien). 2012. PMID: 22426820
-
Surgical management of jugular foramen meningiomas: a series of 13 cases and review of the literature.Laryngoscope. 2007 Oct;117(10):1710-9. doi: 10.1097/MLG.0b013e3180cc20a3. Laryngoscope. 2007. PMID: 17690614 Review.
-
Long-term surgical outcomes of spinal meningiomas.Spine (Phila Pa 1976). 2012 May 1;37(10):E617-23. doi: 10.1097/BRS.0b013e31824167f1. Spine (Phila Pa 1976). 2012. PMID: 22146282 Review.
Cited by
-
Quantitative evaluation of neuroradiological and morphometric alteration of inferior Fronto-Occipital Fascicle across different brain tumor histotype: an Italian multicentric study.Acta Neurochir (Wien). 2025 Mar 12;167(1):71. doi: 10.1007/s00701-025-06488-6. Acta Neurochir (Wien). 2025. PMID: 40072663 Free PMC article.
-
The "state of the art" of intraoperative neurophysiological monitoring: An Italian neurosurgical survey.Brain Spine. 2024 Apr 16;4:102796. doi: 10.1016/j.bas.2024.102796. eCollection 2024. Brain Spine. 2024. PMID: 38698806 Free PMC article.
-
Single versus multiple reoperations for recurrent intracranial meningiomas.J Neurooncol. 2024 Jul;168(3):527-535. doi: 10.1007/s11060-024-04673-8. Epub 2024 Apr 24. J Neurooncol. 2024. PMID: 38656725 Free PMC article.
-
Risk factors for motor decline following parasagittal and falx meningioma resection in the middle third.Front Oncol. 2025 Feb 4;15:1458934. doi: 10.3389/fonc.2025.1458934. eCollection 2025. Front Oncol. 2025. PMID: 39968067 Free PMC article.
-
Risk factors on surgical compliance and its impact on survival outcomes in meningioma patients: a SEER-based retrospective propensity-score matched analysis.BMC Surg. 2024 Jan 30;24(1):39. doi: 10.1186/s12893-024-02326-1. BMC Surg. 2024. PMID: 38291417 Free PMC article.
References
-
- Coșman M, Panțiru IM, Cucu A, Atomei AL, Dumitrecu GF, Poeată I. Surgical management of Rolandic area meningioma in the era of intraoperative neurophysiological monitoring. Rom Neurosurg. 2020;XXXIV(4):488–494. doi: 10.33962/roneuro-2020-082. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
