

Profile and quality of life of the adult population in good health according to the level of vitality: European NHWS cross sectional analysis
- PMID: 37277779
- PMCID: PMC10239722
- DOI: 10.1186/s12889-023-15754-0
Profile and quality of life of the adult population in good health according to the level of vitality: European NHWS cross sectional analysis
Abstract
Background: The World Health Organization's definition of health highlights the importance of mental and physical wellbeing and not only disease state. However, lack of awareness on the burden of impaired vitality and its impact on the quality of life of the general healthy population prevents healthcare providers from delivering appropriate solutions and advice. This study aims to better characterize this population in Europe and identify the profile and the health reported outcomes associated with impaired vitality.
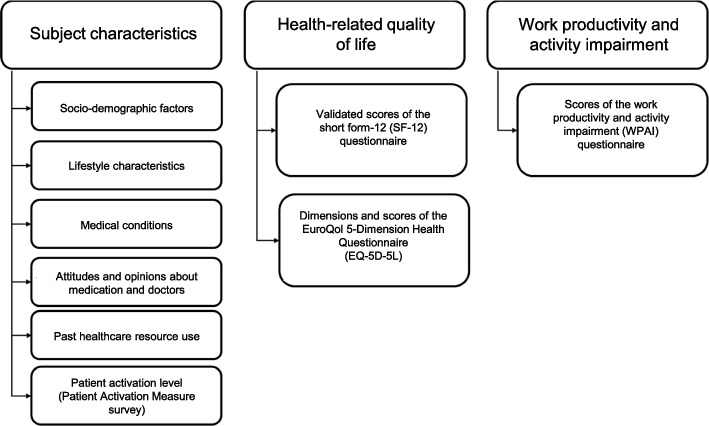
Methods: This retrospective observational study included National Health and Wellness Survey (NHWS) data collected in healthy participants aged 18-65 years from five European Union countries in 2018. Socio-demographic and lifestyle characteristics, comorbidities, attitudes towards healthcare systems, Patient Activation Measure, health-related quality of life outcomes (EQ-5D), and work productivity and activity impairment were analysed according to SF-12 vitality score subgroups (≥ 60, 50- < 60, 40- < 50, < 40).
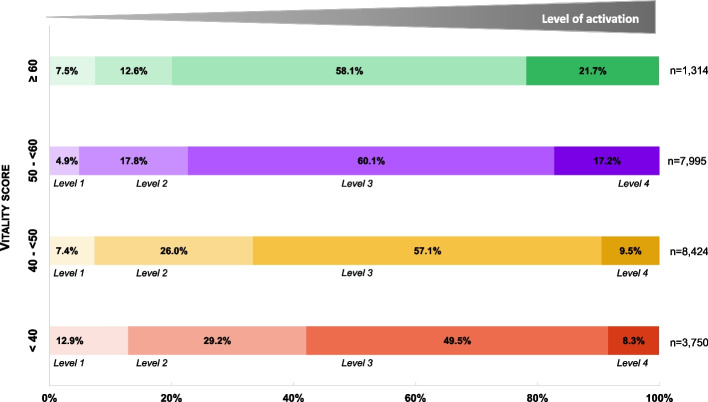
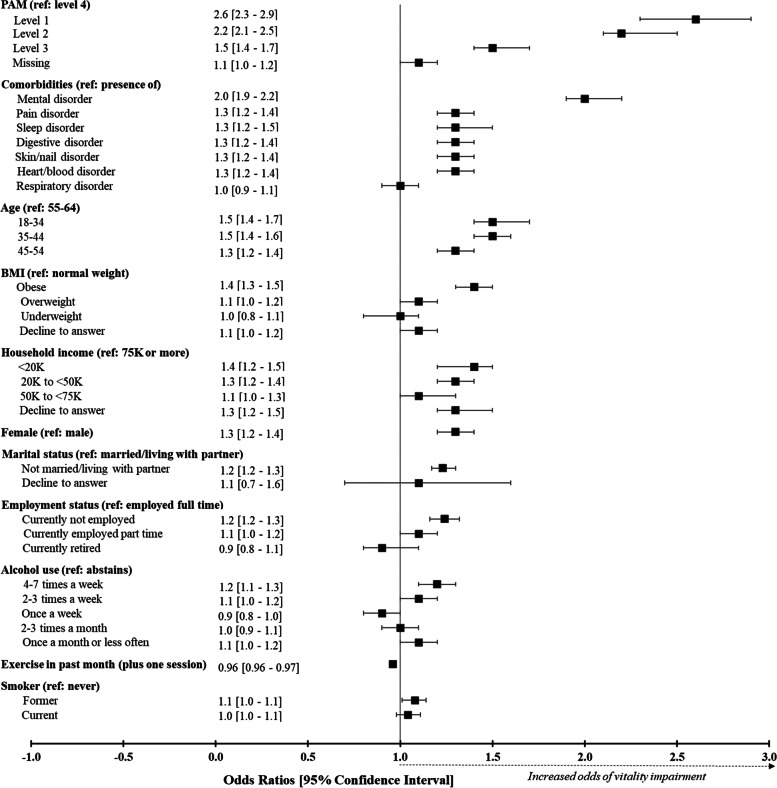
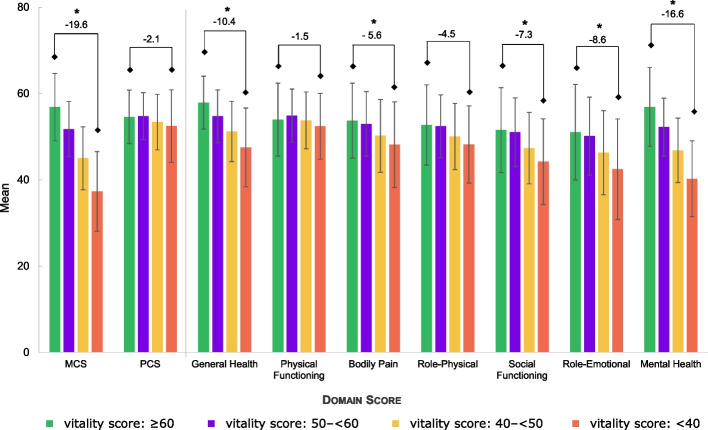
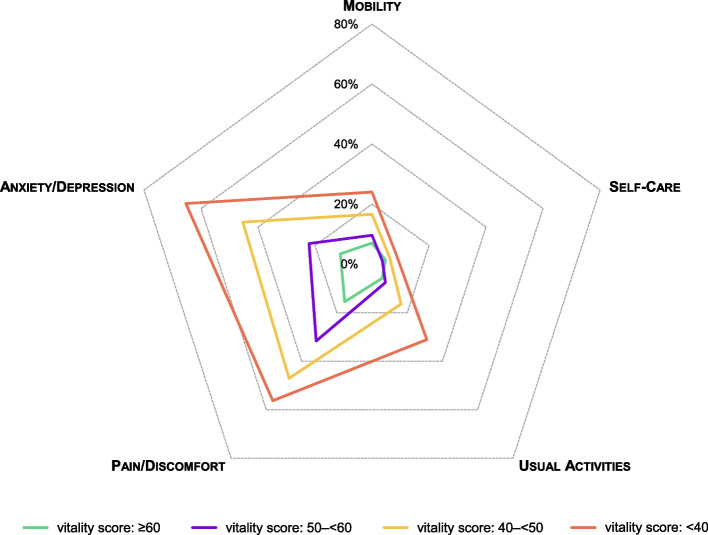
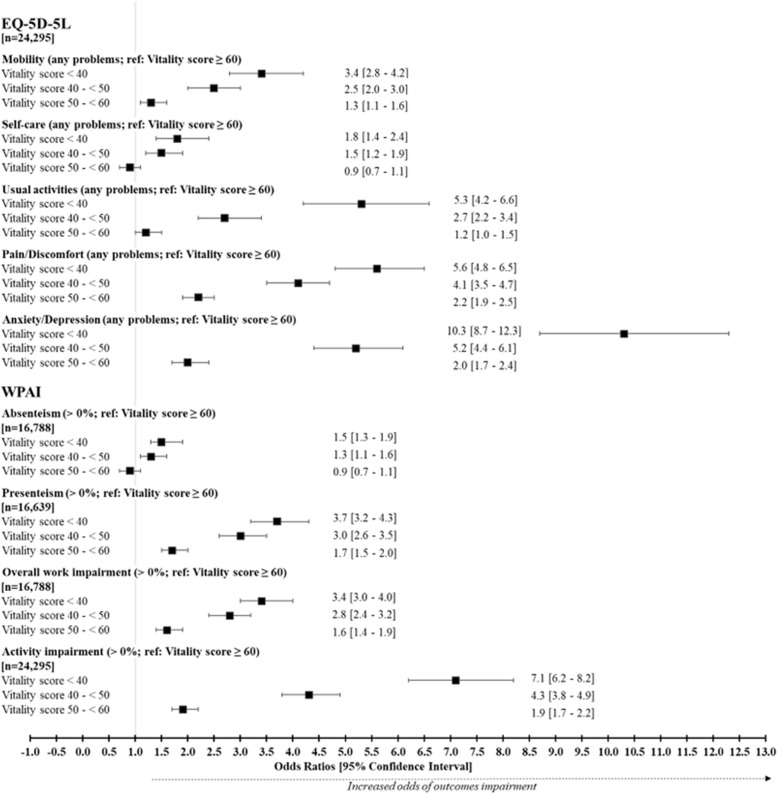
Results: A total of 24,295 participants were enrolled in the main analysis. Being a female, younger, having a lower income and being obese or having sleep and mental disorders was associated with an increased risk of impaired vitality. This was associated with a higher consumption of healthcare resources along with having a weak patient-physician relationship. Participants who were disengaged in the self-management of their health were 2.6 times more likely to have a low level of vitality. For participants in the lowest vitality group, odds of mobility problems increased by 3.4, impairment of usual activity by 5.8, increased of pain and discomfort by 5.6 and depression and anxiety by 10.3, compared with participants in the highest vitality group. Also, odds of presenteeism increased by 3.7, overall work impairment by 3.4 and daily activity losses by 7.1.
Conclusion: Evidence-based trends facilitate the identification of a healthy population with impaired vitality in real-world practice. This study highlights the actual burden of low vitality on daily life activities, particularly on mental health and reduced work productivity. Additionally, our results underline the importance of self-engagement in the management of vitality impairment and highlights the need to implement strategies to address this public health concern in the affected population (HCP-patient communication, supplements, meditation).
Keywords: Fatigue; Good health; Health-related quality of life; NHWS; Patient activation; Patient profile; Vitality.
© 2023. The Author(s).
Conflict of interest statement
Caroline Armand, Andrew Steward and Anne-Laure Tardy are full-time employees of Sanofi Consumer Healthcare.
Sophie Marguet, Halley Costantino and deMauri Mackie are full-time employees of Cerner Enviza (formerly Kantar Health), the organization that received funding from Sanofi Consumer Healthcare for the conduct of this study. Grèce Saba was a full-time employee of Cerner Enviza (formerly Kantar Health) at the time of the study.
The authors report no other conflicts of interest in this work.
Figures

References
-
- Aritake S, Kaneita Y, Ohtsu T, Uchiyama M, Mishima K, Akashiba T, et al. Prevalence of fatigue symptoms and correlations in the general adult population. Sleep Biol Rhythms. 2015;13(2):146–154. doi: 10.1111/sbr.12099. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
