

Emerging Perspectives on MRI Application in Multiple Sclerosis: Moving from Pathophysiology to Clinical Practice
- PMID: 37278626
- PMCID: PMC10315528
- DOI: 10.1148/radiol.221512
Emerging Perspectives on MRI Application in Multiple Sclerosis: Moving from Pathophysiology to Clinical Practice
Abstract
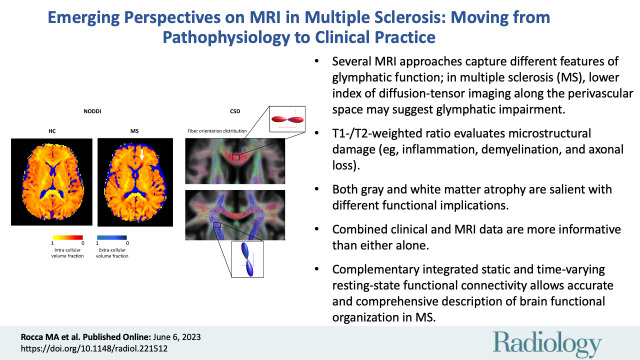
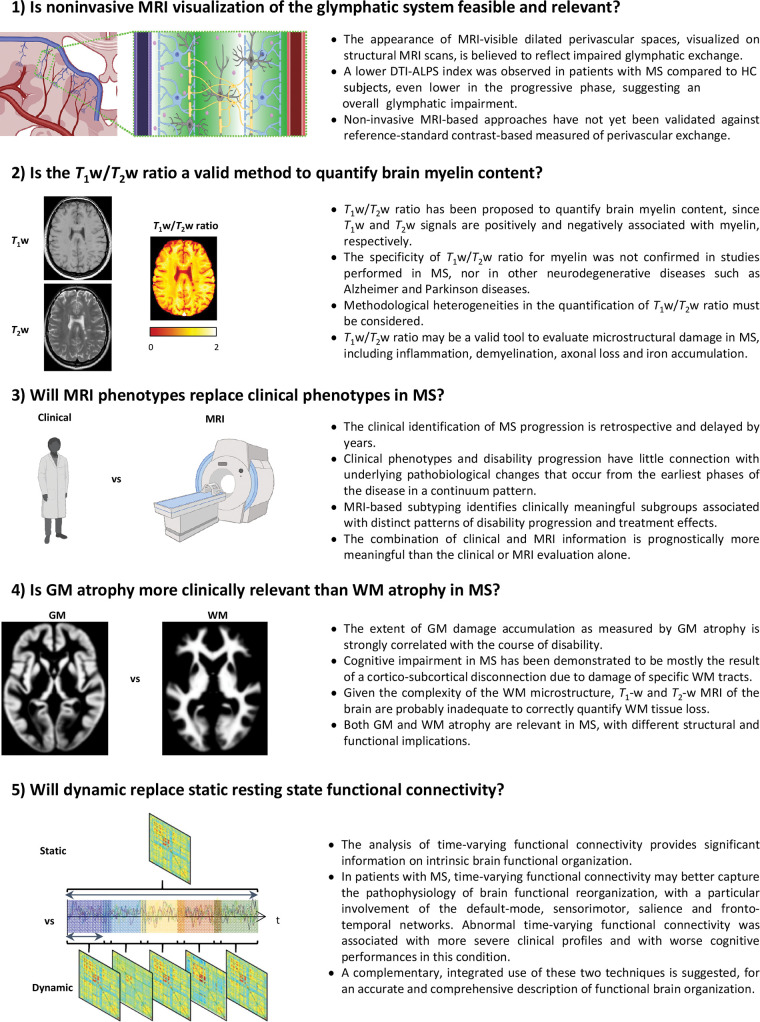
MRI plays a central role in the diagnosis of multiple sclerosis (MS) and in the monitoring of disease course and treatment response. Advanced MRI techniques have shed light on MS biology and facilitated the search for neuroimaging markers that may be applicable in clinical practice. MRI has led to improvements in the accuracy of MS diagnosis and a deeper understanding of disease progression. This has also resulted in a plethora of potential MRI markers, the importance and validity of which remain to be proven. Here, five recent emerging perspectives arising from the use of MRI in MS, from pathophysiology to clinical application, will be discussed. These are the feasibility of noninvasive MRI-based approaches to measure glymphatic function and its impairment; T1-weighted to T2-weighted intensity ratio to quantify myelin content; classification of MS phenotypes based on their MRI features rather than on their clinical features; clinical relevance of gray matter atrophy versus white matter atrophy; and time-varying versus static resting-state functional connectivity in evaluating brain functional organization. These topics are critically discussed, which may guide future applications in the field.
© RSNA, 2023.
Conflict of interest statement
Figures





References
-
- Filippi M , Bar-Or A , Piehl F , et al. . Multiple sclerosis . Nat Rev Dis Primers 2018. ; 4 ( 1 ): 43 . [Published correction appears in Nat Rev Dis Primers 2018;4(1):49.] - PubMed
-
- Filippi M , Preziosa P , Rocca MA . MRI in multiple sclerosis: what is changing? Curr Opin Neurol 2018. ; 31 ( 4 ): 386 – 395 . - PubMed
-
- Zhou Y , Cai J , Zhang W , et al. . Impairment of the Glymphatic Pathway and Putative Meningeal Lymphatic Vessels in the Aging Human . Ann Neurol 2020. ; 87 ( 3 ): 357 – 369 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
