

Molecular diagnostic tools for the World Health Organization (WHO) 2021 classification of gliomas, glioneuronal and neuronal tumors; an EANO guideline
- PMID: 37279174
- PMCID: PMC10547522
- DOI: 10.1093/neuonc/noad100
Molecular diagnostic tools for the World Health Organization (WHO) 2021 classification of gliomas, glioneuronal and neuronal tumors; an EANO guideline
Abstract
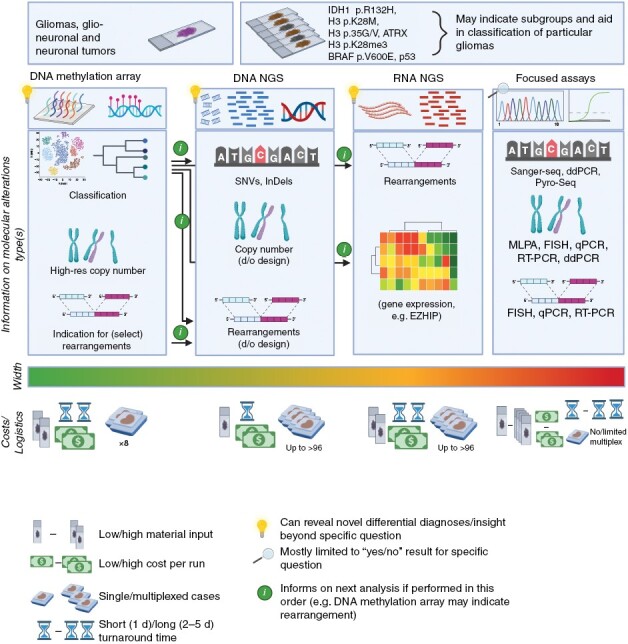
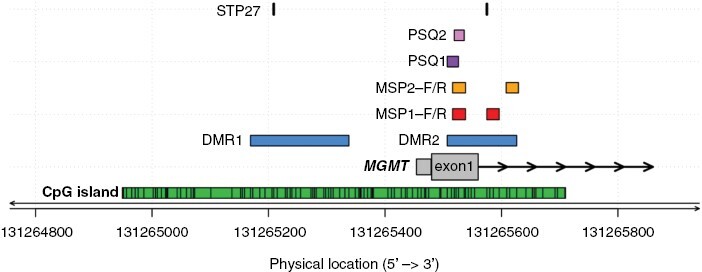
In the 5th edition of the WHO CNS tumor classification (CNS5, 2021), multiple molecular characteristics became essential diagnostic criteria for many additional CNS tumor types. For those tumors, an integrated, "histomolecular" diagnosis is required. A variety of approaches exists for determining the status of the underlying molecular markers. The present guideline focuses on the methods that can be used for assessment of the currently most informative diagnostic and prognostic molecular markers for the diagnosis of gliomas, glioneuronal and neuronal tumors. The main characteristics of the molecular methods are systematically discussed, followed by recommendations and information on available evidence levels for diagnostic measures. The recommendations cover DNA and RNA next-generation-sequencing, methylome profiling, and select assays for single/limited target analyses, including immunohistochemistry. Additionally, because of its importance as a predictive marker in IDH-wildtype glioblastomas, tools for the analysis of MGMT promoter methylation status are covered. A structured overview of the different assays with their characteristics, especially their advantages and limitations, is provided, and requirements for input material and reporting of results are clarified. General aspects of molecular diagnostic testing regarding clinical relevance, accessibility, cost, implementation, regulatory, and ethical aspects are discussed as well. Finally, we provide an outlook on new developments in the landscape of molecular testing technologies in neuro-oncology.
Keywords: WHO classification; glioma; glioneuronal tumors; molecular classification; molecular diagnostics; neuronal tumors.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
Comment in
-
Advanced molecular diagnostic tools: A step closer to precision medicine in neuro-oncology.Neuro Oncol. 2023 Oct 3;25(10):1750-1751. doi: 10.1093/neuonc/noad132. Neuro Oncol. 2023. PMID: 37503808 Free PMC article. No abstract available.
References
-
- Wesseling P, Capper D.. WHO 2016 Classification of gliomas. Neuropathol Appl Neurobiol. 2018;44(2):139–150. - PubMed
-
- Coons SW, Johnson PC, Scheithauer BW, Yates AJ, Pearl DK.. Improving diagnostic accuracy and interobserver concordance in the classification and grading of primary gliomas. Cancer. 1997;79(7):1381–1393. - PubMed
-
- Kros JM, Gorlia T, Kouwenhoven MC, et al. . Panel review of anaplastic oligodendroglioma from European Organization For Research and Treatment of Cancer Trial 26951: assessment of consensus in diagnosis, influence of 1p/19q loss, and correlations with outcome. J Neuropathol Exp Neurol. 2007;66(6):545–551. - PubMed
-
- Kros JM. From expert opinion to evidence-based: changes in the gold standard of primary brain tumour diagnosis. J Pathol. 2007;213(1):1–3. - PubMed
