

Letermovir vs Valganciclovir for Prophylaxis of Cytomegalovirus in High-Risk Kidney Transplant Recipients: A Randomized Clinical Trial
- PMID: 37279999
- PMCID: PMC10245286
- DOI: 10.1001/jama.2023.9106
Letermovir vs Valganciclovir for Prophylaxis of Cytomegalovirus in High-Risk Kidney Transplant Recipients: A Randomized Clinical Trial
Abstract
Importance: Valganciclovir for 200 days is standard care for cytomegalovirus (CMV) prophylaxis in high-risk CMV-seronegative kidney transplant recipients who receive an organ from a CMV-seropositive donor, but its use is limited by myelosuppression.
Objective: To compare the efficacy and safety of letermovir with valganciclovir for prevention of CMV disease in CMV-seronegative kidney transplant recipients who receive an organ from a CMV-seropositive donor.
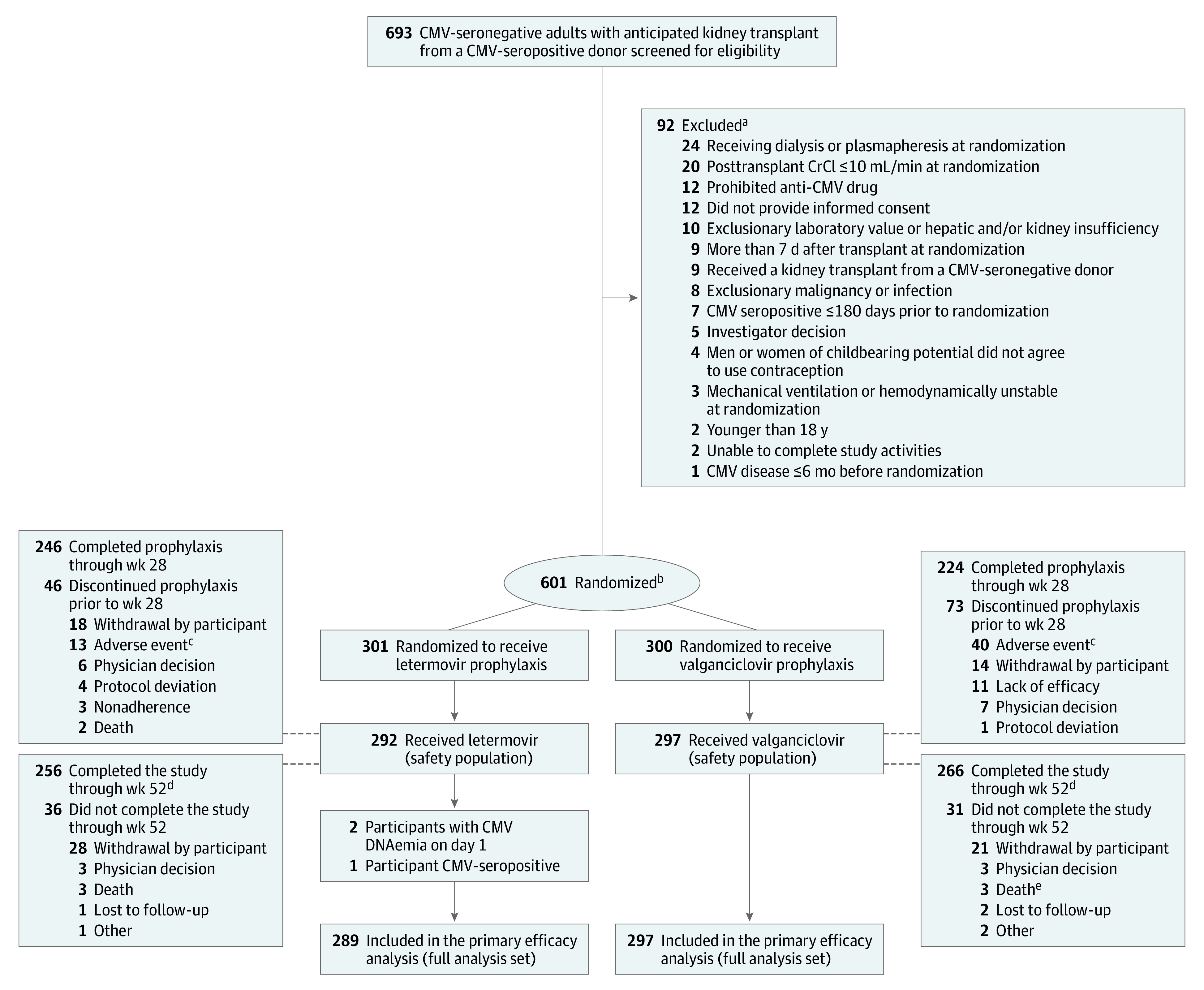
Design, setting, and participants: Randomized, double-masked, double-dummy, noninferiority, phase 3 trial in adult CMV-seronegative kidney transplant recipients who received an organ from a CMV-seropositive donor at 94 participating sites between May 2018 and April 2021 (final follow-up in April 2022).
Interventions: Participants were randomized in a 1:1 ratio (stratified by receipt of lymphocyte-depleting induction immunosuppression) to receive letermovir, 480 mg, orally daily (with acyclovir) or valganciclovir, 900 mg, orally daily (adjusted for kidney function) for up to 200 days after transplant, with matching placebos.
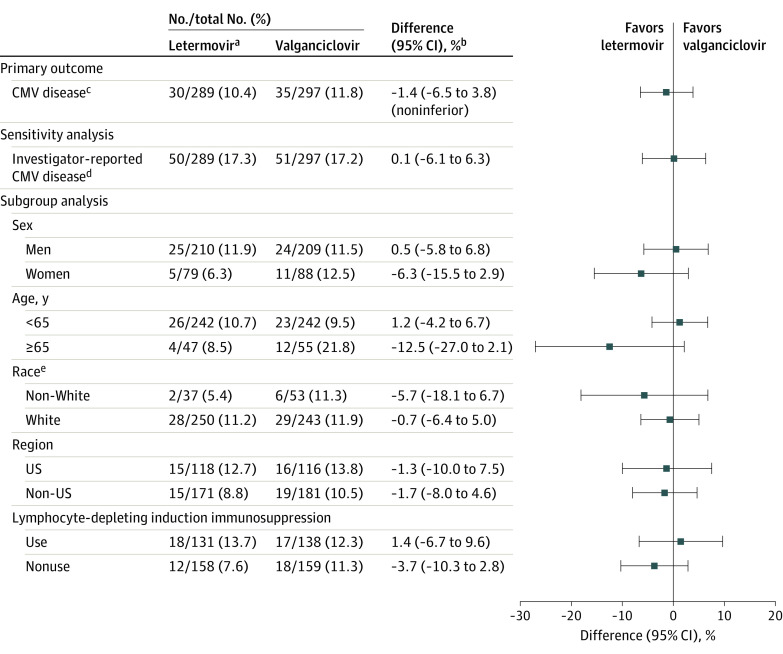
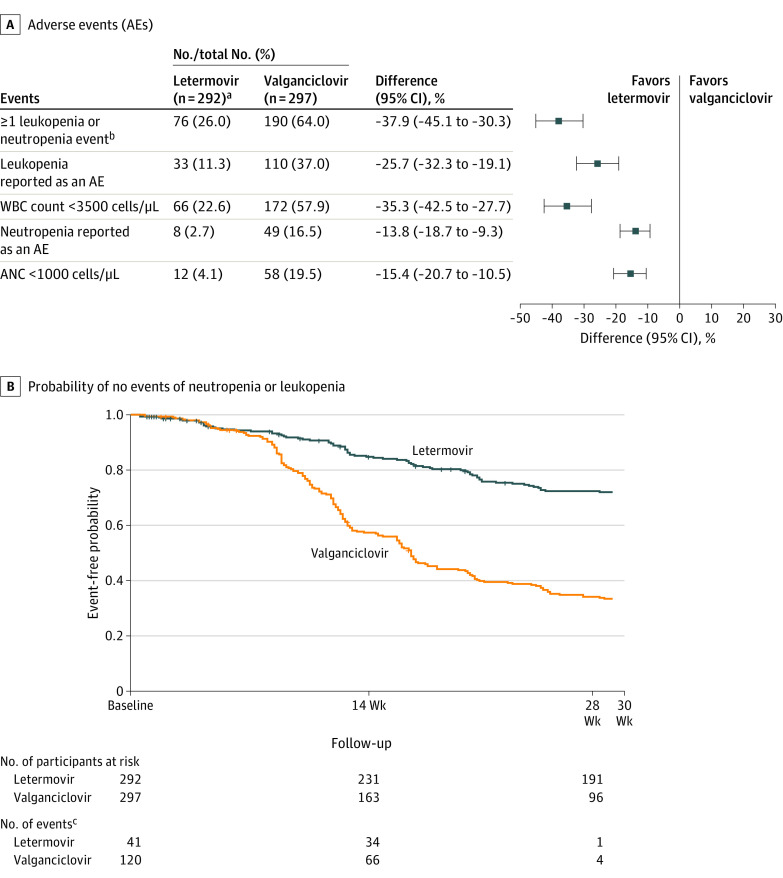
Main outcomes and measures: The primary outcome was CMV disease, confirmed by an independent masked adjudication committee, through posttransplant week 52 (prespecified noninferiority margin, 10%). CMV disease through week 28 and time to onset of CMV disease through week 52 were secondary outcomes. Exploratory outcomes included quantifiable CMV DNAemia and resistance. The rate of leukopenia or neutropenia through week 28 was a prespecified safety outcome.
Results: Among 601 participants randomized, 589 received at least 1 dose of the study drug (mean age, 49.6 years; 422 [71.6%] men). Letermovir (n = 289) was noninferior to valganciclovir (n = 297) for prevention of CMV disease through week 52 (10.4% vs 11.8% of participants with committee-confirmed CMV disease; stratum-adjusted difference -1.4% [95% CI, -6.5% to 3.8%]). No participants who received letermovir vs 5 participants (1.7%) who received valganciclovir developed CMV disease through week 28. Time to onset of CMV disease was comparable between the groups (hazard ratio, 0.90 [95% CI, 0.56-1.47]). Quantifiable CMV DNAemia was detected in 2.1% of participants in the letermovir group vs 8.8% in the valganciclovir group by week 28. Of participants evaluated for suspected CMV disease or CMV DNAemia, none (0/52) who received letermovir and 12.1% (8/66) who received valganciclovir had resistance-associated substitutions. The rate of leukopenia or neutropenia through week 28 was lower with letermovir vs valganciclovir (26% vs 64%; difference, -37.9% [95% CI, -45.1% to -30.3%]; P < .001). Fewer participants in the letermovir group than the valganciclovir group discontinued prophylaxis due to adverse events (4.1% vs 13.5%) or drug-related adverse events (2.7% vs 8.8%).
Conclusion and relevance: Among adult CMV-seronegative kidney transplant recipients who received an organ from a CMV-seropositive donor, letermovir was noninferior to valganciclovir for prophylaxis of CMV disease over 52 weeks, with lower rates of leukopenia or neutropenia, supporting its use for this indication.
Trial registration: ClinicalTrials.gov Identifier: NCT03443869; EudraCT: 2017-001055-30.
Conflict of interest statement
Figures
Comment in
-
A New Antiviral Option for Cytomegalovirus Prevention After Kidney Transplant.JAMA. 2023 Jul 3;330(1):27-29. doi: 10.1001/jama.2023.9100. JAMA. 2023. PMID: 37279971 No abstract available.
-
Letermovir vs Valganciclovir for Cytomegalovirus Prophylaxis After Kidney Transplant.JAMA. 2023 Nov 14;330(18):1802-1803. doi: 10.1001/jama.2023.18022. JAMA. 2023. PMID: 37962657 No abstract available.
-
Letermovir vs Valganciclovir for Cytomegalovirus Prophylaxis After Kidney Transplant.JAMA. 2023 Nov 14;330(18):1803. doi: 10.1001/jama.2023.18019. JAMA. 2023. PMID: 37962658 No abstract available.
References
-
- Kotton CN, Kumar D, Caliendo AM, et al. ; The Transplantation Society International CMV Consensus Group . The third International Consensus Guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. 2018;102(6):900-931. doi: 10.1097/TP.0000000000002191 - DOI - PubMed
-
- Paya C, Humar A, Dominguez E, et al. ; Valganciclovir Solid Organ Transplant Study Group . Efficacy and safety of valganciclovir vs oral ganciclovir for prevention of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant. 2004;4(4):611-620. doi: 10.1111/j.1600-6143.2004.00382.x - DOI - PubMed
