

Tolerability of bedtime diuretics: a prospective cohort analysis
- PMID: 37280022
- PMCID: PMC10255011
- DOI: 10.1136/bmjopen-2022-068188
Tolerability of bedtime diuretics: a prospective cohort analysis
Abstract
Objectives: We sought to validate, or refute, the common belief that bedtime diuretics are poorly tolerated due to nocturia.
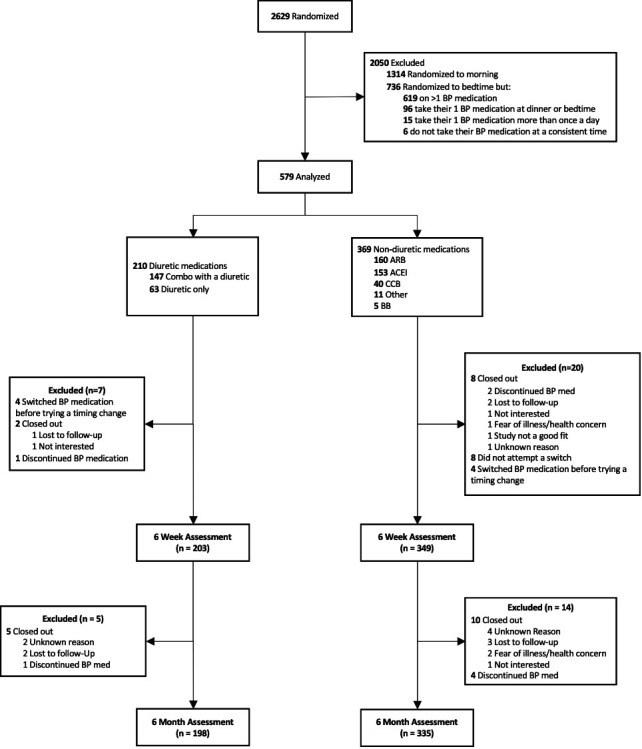
Design: Prespecified prospective cohort analysis embedded within the randomised BedMed trial, in which hypertensive participants are randomised to morning versus bedtime antihypertensive administration.
Setting: 352 community family practices across 4 Canadian provinces between March 2017 and September 2020.
Participants: 552 hypertensive patients (65.6 years old, 57.4% female) already established on a single once-daily morning antihypertensive and randomised to switch that antihypertensive to bedtime. Of these, 203 used diuretics (27.1% thiazide alone, 70.0% thiazide/non-diuretic combinations) and 349 used non-diuretics.
Intervention: Switching the established antihypertensive from morning to bedtime, and comparing the experience of diuretic and non-diuretic users.
Primary and secondary outcome measures: Primary outcome: Adherence to bedtime allocation time at 6 months (defined as the willingness to continue with bedtime use, not an assessment of missed doses). Secondary 6-month outcomes: (1) nocturia considered to be a major burden and (2) increase in overnight urinations/week. All outcomes were self-reported and additionally collected at 6 weeks.
Results: At 6 months: Adherence to bedtime allocation time was lower in diuretic users than non-diuretic users (77.3% vs 89.8%; difference 12.6%; 95% CI 5.8% to 19.8%; p<0.0001; NNH 8.0), and more diuretic users considered nocturia a major burden (15.6% vs 1.3%; difference 14.2%; 95% CI 8.9% to 20.6%; p<0.0001; NNH 7.0). Compared with baseline, diuretic users experienced 1.0 more overnight urinations/week (95% CI 0.0 to 1.75; p=0.01). Results did not differ between sexes.
Conclusions: Switching diuretics to bedtime did promote nocturia, but only 15.6% found nocturia a major burden. At 6 months, 77.3% of diuretic users were adherent to bedtime dosing. Bedtime diuretic use is viable for many hypertensive patients, should it ever become clinically indicated.
Trial registration number: NCT02990663.
Keywords: CLINICAL PHARMACOLOGY; Cardiology; Hypertension; PRIMARY CARE.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: SRG is the nominated principal applicant of two grants from governmental sources that are funding the BedMed trial (from Alberta Innovates, and the Canadian Institutes of Health Research); RSP is CEO of 'mmHg', a digital health company and maker of software solutions for BP monitoring; MDH is the recipient of several grants from pharmaceutical and device companies related to interventions geared at stroke treatment. He holds two device patents related to stroke imaging, has chaired or sat on the data safety monitoring boards of five other cardiovascular trials, is the President of the Canadian Neurological Sciences Federation, a member of the board of the Canadian Stroke Consortium, and has private stock ownership in two companies targeting imaging interventions (Circle and PureWeb).
Figures

References
-
- Carlsberg B, Brunstrom B. Is bedtime the best time of day? International society of hypertension March 2020 newsletter. Available: https://ish-world.com/data/uploads/2003-1.pdf#page=19 [Accessed 17 Dec 2021].
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical