

Amyloid-related imaging abnormalities (ARIA): radiological, biological and clinical characteristics
- PMID: 37280110
- PMCID: PMC10629981
- DOI: 10.1093/brain/awad188
Amyloid-related imaging abnormalities (ARIA): radiological, biological and clinical characteristics
Abstract
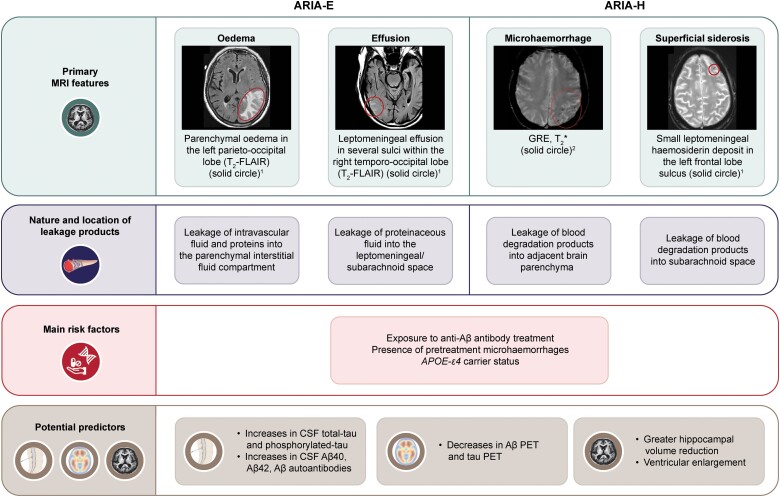
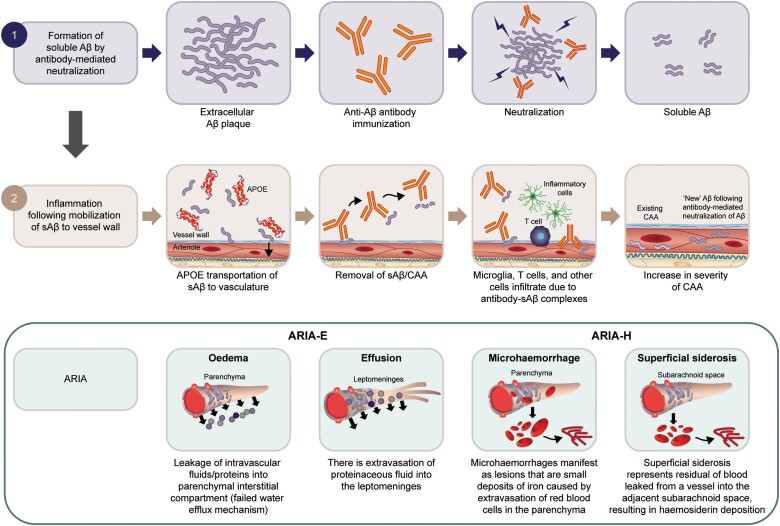
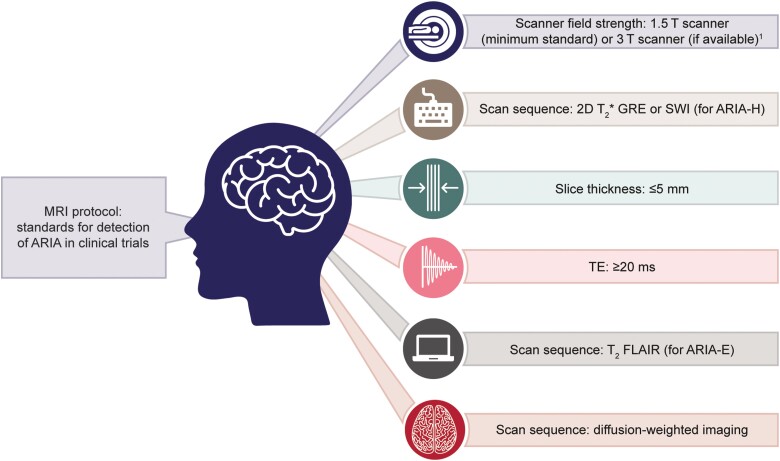
Excess accumulation and aggregation of toxic soluble and insoluble amyloid-β species in the brain are a major hallmark of Alzheimer's disease. Randomized clinical trials show reduced brain amyloid-β deposits using monoclonal antibodies that target amyloid-β and have identified MRI signal abnormalities called amyloid-related imaging abnormalities (ARIA) as possible spontaneous or treatment-related adverse events. This review provides a comprehensive state-of-the-art conceptual review of radiological features, clinical detection and classification challenges, pathophysiology, underlying biological mechanism(s) and risk factors/predictors associated with ARIA. We summarize the existing literature and current lines of evidence with ARIA-oedema/effusion (ARIA-E) and ARIA-haemosiderosis/microhaemorrhages (ARIA-H) seen across anti-amyloid clinical trials and therapeutic development. Both forms of ARIA may occur, often early, during anti-amyloid-β monoclonal antibody treatment. Across randomized controlled trials, most ARIA cases were asymptomatic. Symptomatic ARIA-E cases often occurred at higher doses and resolved within 3-4 months or upon treatment cessation. Apolipoprotein E haplotype and treatment dosage are major risk factors for ARIA-E and ARIA-H. Presence of any microhaemorrhage on baseline MRI increases the risk of ARIA. ARIA shares many clinical, biological and pathophysiological features with Alzheimer's disease and cerebral amyloid angiopathy. There is a great need to conceptually link the evident synergistic interplay associated with such underlying conditions to allow clinicians and researchers to further understand, deliberate and investigate on the combined effects of these multiple pathophysiological processes. Moreover, this review article aims to better assist clinicians in detection (either observed via symptoms or visually on MRI), management based on appropriate use recommendations, and general preparedness and awareness when ARIA are observed as well as researchers in the fundamental understanding of the various antibodies in development and their associated risks of ARIA. To facilitate ARIA detection in clinical trials and clinical practice, we recommend the implementation of standardized MRI protocols and rigorous reporting standards. With the availability of approved amyloid-β therapies in the clinic, standardized and rigorous clinical and radiological monitoring and management protocols are required to effectively detect, monitor, and manage ARIA in real-world clinical settings.
Keywords: Alzheimer’s disease; amyloid-related imaging abnormalities; anti-amyloid monoclonal antibodies; cerebral amyloid angiopathy; disease-modifying therapies.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
H.H. is an employee of Eisai Inc. He serves as Reviewing Editor for the Journal Alzheimer’s and Dementia and does not receive any fees or honoraria since May 2019. He is inventor of 11 patents and has received no royalties: (i) In Vitro Multiparameter Determination Method for The Diagnosis and Early Diagnosis of Neurodegenerative Disorders Patent Number: 8916388; (ii) In Vitro Procedure for Diagnosis and Early Diagnosis of Neurodegenerative Diseases Patent Number: 8298784; (iii) Neurodegenerative Markers for Psychiatric Conditions Publication Number: 20120196300; (iv) In Vitro Multiparameter Determination Method for The Diagnosis and Early Diagnosis of Neurodegenerative Disorders Publication Number: 20100062463; (v) In Vitro Method for The Diagnosis and Early Diagnosis of Neurodegenerative Disorders Publication Number: 20100035286; (vi) In Vitro Procedure for Diagnosis and Early Diagnosis of Neurodegenerative Diseases Publication Number: 20090263822; (vii) In Vitro Method for The Diagnosis of Neurodegenerative Diseases Patent Number: 7547553; (viii) CSF Diagnostic in Vitro Method for Diagnosis of Dementias and Neuroinflammatory Diseases Publication Number: 20080206797; (ix) In Vitro Method for The Diagnosis of Neurodegenerative Diseases Publication Number: 20080199966; (x) Neurodegenerative Markers for Psychiatric Conditions Publication Number: 20080131921; and (xi) Method for diagnosis of dementias and neuroinflammatory diseases based on an increased level of procalcitonin in cerebrospinal fluid: Publication number: United States Patent 10921330. A.A. has received in the past 10 years, or may receive, honoraria for consulting; participating in independent data safety monitoring boards; providing educational lectures, programs, and materials; or serving on advisory boards for AbbVie, Acadia, Allergan, the Alzheimer’s Association, Axovant, AZ Therapies, Biogen, Eisai, Grifols, Harvard Medical School Graduate Continuing Education, JOMDD, Lundbeck, Merck, Roche/Genentech, Novo Nordisk, Qynapse, Sunovion, Suven, and Synexus. A.A. receives book royalties from Oxford University Press for a medical book on dementia. A.A. receives institutional research grant/contract funding from NIA/NIH 1P30AG072980, AZ DHS CTR040636, Washington University St Louis, and Gates Ventures. A.A.’s institution receives/received funding for clinical trial grants, contracts and projects from government, consortia, foundations, and companies for which he serves/served as contracted site PI. A.A., at his previous institution, served as site PI for the Biogen EMERGE study; and, at his current institution, serves as site PI for the ACTC-Eisai AHEAD 3–45 study (clinical trial contract with institution). L.G.A. receives research support from NIH, Alzheimer Association, AVID Pharmaceuticals, Life Molecular Imaging, Roche Diagnostics. L.G.A. has served as a consultant for Biogen, Two Labs, IQVIA, NIH, Florida Dept. Health, NIH Biobank, Eli Lilly, Eisai, GE Healthcare, Roche Diagnostics, and Genentech. L.G.A. is a member of various data and safety monitoring boards (DSMBs) and advisory boards for IQVIA, NIA R01 AG061111, UAB Nathan Schick Center, FDA PCNS Advisory Board, University New Mexico ADRC. L.G.A. owns stock in Cassava Neurosciences. J.A.R.N. has been consultant/advisor relating to Alzheimer immunotherapy programmes for Elan Pharmaceuticals, GlaxoSmithKline, Novartis, Roche, Janssen, Pfizer and Biogen. M.C. and A.E. are employees of Eisai Inc.
Figures
References
-
- Dubois B, Feldman HH, Jacova C, et al. Advancing research diagnostic criteria for Alzheimer's disease: The IWG-2 criteria. Lancet Neurol. 2014;13:614–629. - PubMed
-
- Karran E, De Strooper B. The amyloid hypothesis in Alzheimer disease: New insights from new therapeutics. Nat Rev Drug Discov. 2022;21:306–318. - PubMed
-
- Hampel H, Cummings J, Blennow K, Gao P, Jack C, Vergallo A. Developing the ATX(N) classification for use across the Alzheimer disease continuum. Nat Rev Neurol. 2021;17:580–589. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
