

Histological transformation to signet-ring cell carcinoma in a patient with clinically aggressive poorly differentiated adenocarcinoma of the ascending colon after response to chemotherapy plus cetuximab: a case report
- PMID: 37280577
- PMCID: PMC10245628
- DOI: 10.1186/s12957-023-03053-2
Histological transformation to signet-ring cell carcinoma in a patient with clinically aggressive poorly differentiated adenocarcinoma of the ascending colon after response to chemotherapy plus cetuximab: a case report
Abstract
Background: Alteration of chemosensitivity or tumor aggressiveness in response to chemotherapy has been reported, and liquid biopsy assessment during chemotherapy for colorectal cancers has confirmed the acquisition of mutations in various oncogenes. However, the occurrence of histological transformation seems to be extremely rare in colorectal cancers, and the few existing case reports of this transformation are from lung cancer and breast cancer. In this report, we describe the histological transformation of clinically aggressive scirrhous-type poorly differentiated adenocarcinoma of the ascending colon to signet-ring cell carcinoma in almost all recurrent tumors that were confirmed by autopsy after response to chemotherapy plus cetuximab.
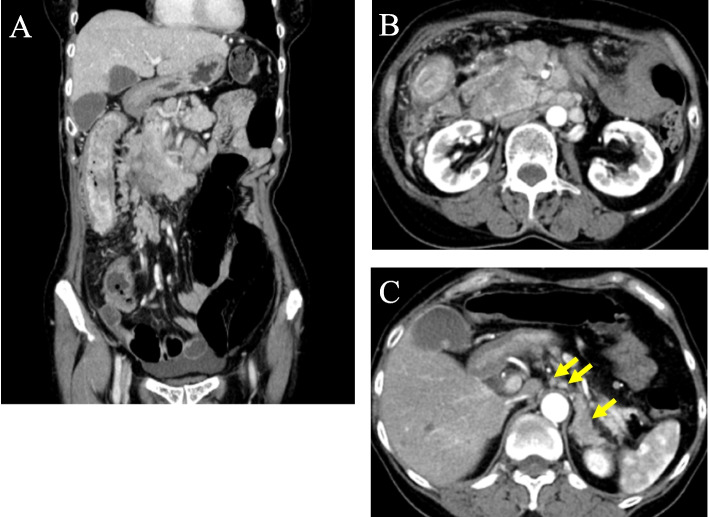
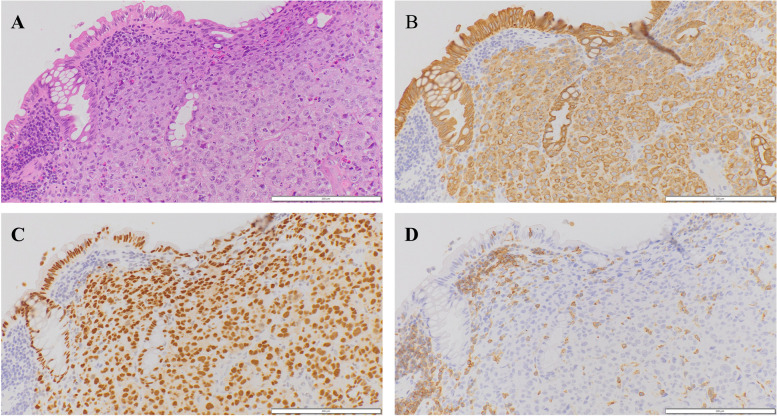
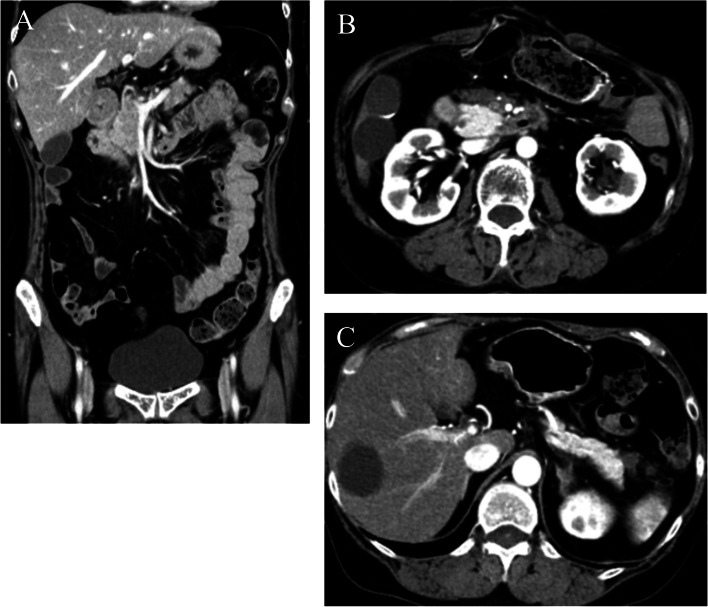
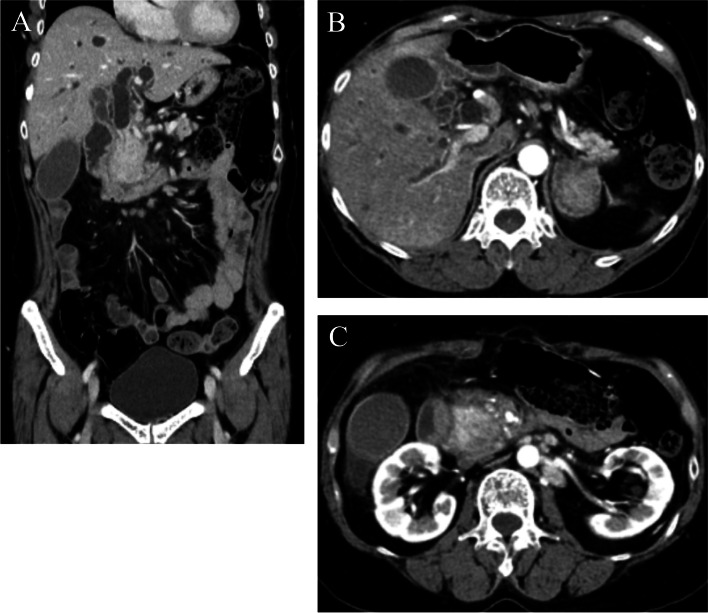
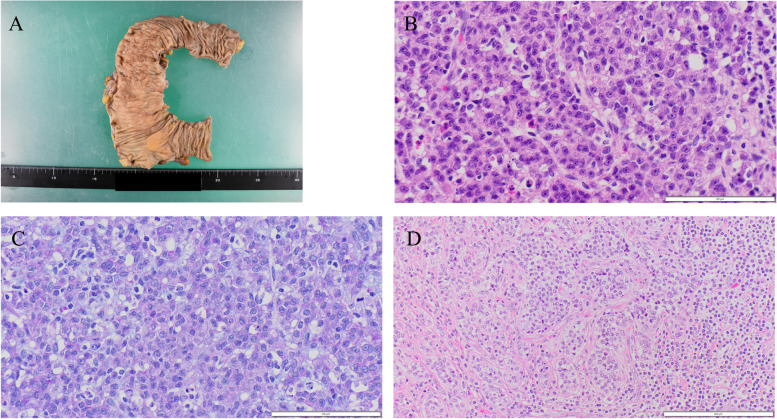
Case presentation: A 59-year-old woman visited our hospital with whole abdominal pain and body weight loss and was diagnosed with scirrhous-type poorly differentiated adenocarcinoma of the ascending colon with aggressive lymph node metastases. The intrinsic chemosensitivity of the tumors was evident upon initiation of mFOLFOX6 plus cetuximab therapy, and right hemicolectomy was performed, and the tumor obviously remained in the peripancreatic area, paraaortic region, or other retroperitoneal areas. The ascending colon tumors mainly consisted of poorly differentiated adenocarcinoma and were not associated with signet-ring cell components except for minute clusters in a few lymphatic emboli in the main tumor. Chemotherapy was continued, and metastases were eliminated at 8 months after the operation; this response was maintained for an additional 4 months. Discontinuation of chemotherapy plus cetuximab resulted in immediate tumor recurrence and rapid expansion, and the patient died of the recurrent tumor 1 year and 2 months after the operation. Autopsy specimens revealed that almost all of the recurrent tumors exhibited transformation and consisted of signet-ring cell histology.
Conclusion: This case might suggest that various oncogene mutations or epigenetic changes resulting from chemotherapy, especially regimens that include cetuximab, contribute to the transformation of non-signet-ring cell colorectal carcinoma to signet-ring cell carcinoma histology and can promote the aggressive clinical progression characteristic of signet-ring cell carcinoma.
Keywords: Ascending colon cancer; Cetuximab; Chemotherapy; Histological transformation; Poorly differentiated adenocarcinoma; Signet-ring cell carcinoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
