

Variability in white blood cell count during uncomplicated malaria and implications for parasite density estimation: a WorldWide Antimalarial Resistance Network individual patient data meta-analysis
- PMID: 37280686
- PMCID: PMC10243075
- DOI: 10.1186/s12936-023-04583-6
Variability in white blood cell count during uncomplicated malaria and implications for parasite density estimation: a WorldWide Antimalarial Resistance Network individual patient data meta-analysis
Abstract
Background: The World Health Organization (WHO) recommends that when peripheral malarial parasitaemia is quantified by thick film microscopy, an actual white blood cell (WBC) count from a concurrently collected blood sample is used in calculations. However, in resource-limited settings an assumed WBC count is often used instead. The aim of this study was to describe the variability in WBC count during acute uncomplicated malaria, and estimate the impact of using an assumed value of WBC on estimates of parasite density and clearance.
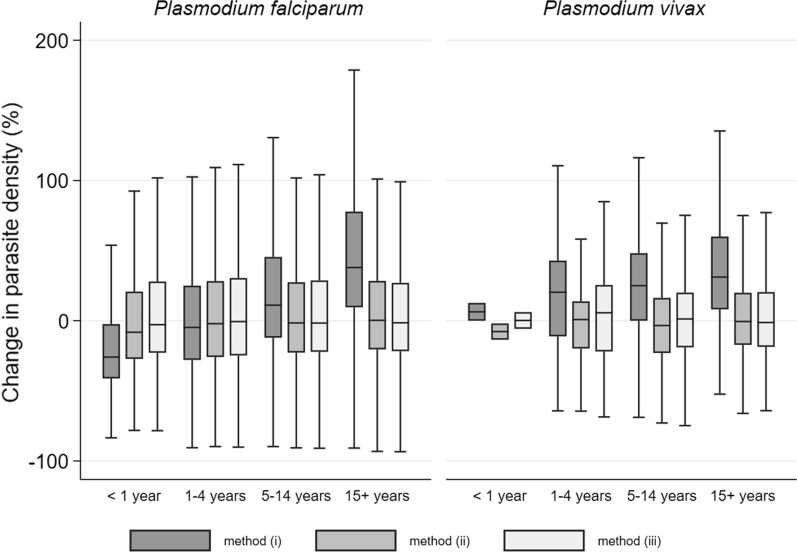
Methods: Uncomplicated malaria drug efficacy studies that measured WBC count were selected from the WorldWide Antimalarial Resistance Network data repository for an individual patient data meta-analysis of WBC counts. Regression models with random intercepts for study-site were used to assess WBC count variability at presentation and during follow-up. Inflation factors for parasitaemia density, and clearance estimates were calculated for methods using assumed WBC counts (8000 cells/µL and age-stratified values) using estimates derived from the measured WBC value as reference.
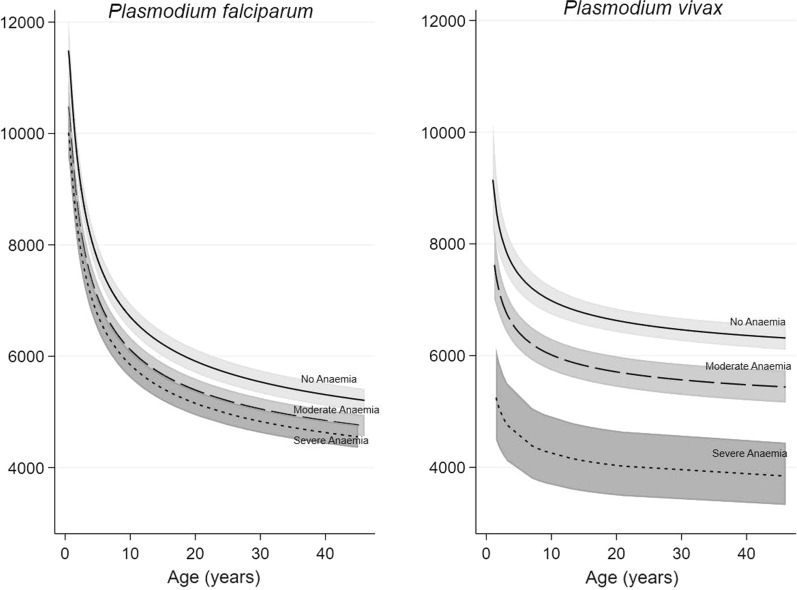
Results: Eighty-four studies enrolling 27,656 patients with clinically uncomplicated malaria were included. Geometric mean WBC counts (× 1000 cells/µL) in age groups < 1, 1-4, 5-14 and ≥ 15 years were 10.5, 8.3, 7.1, 5.7 and 7.5, 7.0, 6.5, 6.0 for individuals with falciparum (n = 24,978) and vivax (n = 2678) malaria, respectively. At presentation, higher WBC counts were seen among patients with higher parasitaemia, severe anaemia and, for individuals with vivax malaria, in regions with shorter regional relapse periodicity. Among falciparum malaria patients, using an assumed WBC count of 8000 cells/µL resulted in parasite density underestimation by a median (IQR) of 26% (4-41%) in infants < 1 year old but an overestimation by 50% (16-91%) in adults aged ≥ 15 years. Use of age-stratified assumed WBC values removed systematic bias but did not improve precision of parasitaemia estimation. Imprecision of parasite clearance estimates was only affected by the within-patient WBC variability over time, and remained < 10% for 79% of patients.
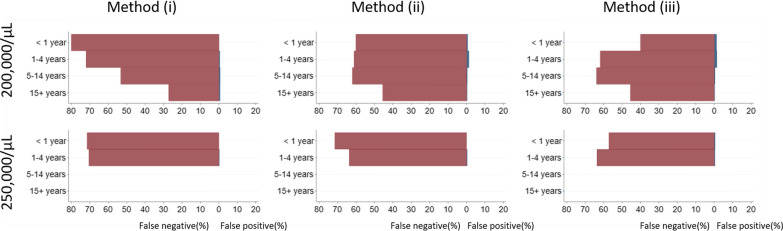
Conclusions: Using an assumed WBC value for parasite density estimation from a thick smear may lead to underdiagnosis of hyperparasitaemia and could adversely affect clinical management; but does not result in clinically consequential inaccuracies in the estimation of the prevalence of prolonged parasite clearance and artemisinin resistance.
Keywords: Leukocyte; Malaria; Microscopy; Parasitaemia; White blood cell.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- WHO . World malaria report 2022. Geneva: World Health Organization; 2023.
-
- Akinosoglou KS, Solomou EE, Gogos CA. Malaria: a haematological disease. Hematol Amst Neth. 2012;17:106–114. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
