

Improvement of synaptic plasticity and cognitive function in RASopathies-a monocentre, randomized, double-blind, parallel-group, placebo-controlled, cross-over clinical trial (SynCoRAS)
- PMID: 37280688
- PMCID: PMC10246096
- DOI: 10.1186/s13063-023-07392-z
Improvement of synaptic plasticity and cognitive function in RASopathies-a monocentre, randomized, double-blind, parallel-group, placebo-controlled, cross-over clinical trial (SynCoRAS)
Abstract
Background: Cognitive impairment is a common medical issue in rat sarcoma (RAS) pathway disorders, so-called RASopathies, like Neurofibromatosis type 1 (NF1) or Noonan syndrome (NS). It is presumed to be caused by impaired synaptic plasticity. In animal studies, pathway-specific pharmacological interventions with lovastatin (LOV) and lamotrigine (LTG) have been shown to improve synaptic plasticity as well as cognitive function. The aim of this clinical trial is to translate the findings of animal studies to humans and to probe the effect of lovastatin (NS) and lamotrigine (NS and NF1) on synaptic plasticity and cognitive function/alertness in RASopathies.
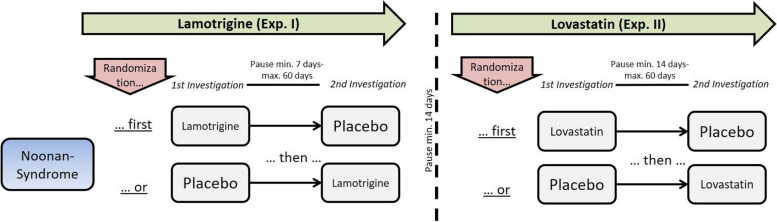
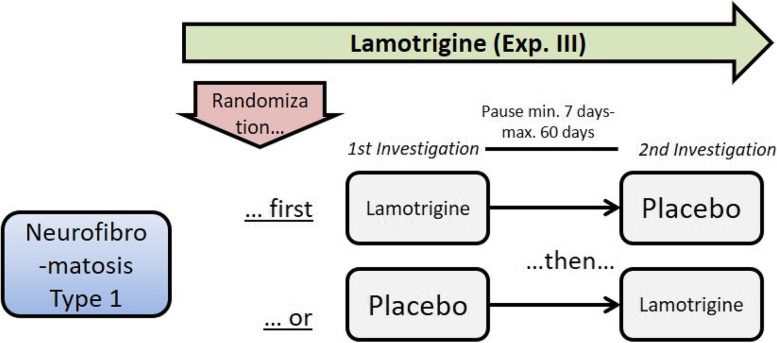
Methods: Within this phase IIa, monocentre, randomized, double-blind, parallel-group, placebo-controlled, cross-over clinical trial (syn. SynCoRAS), three approaches (approaches I-III) will be carried out. In patients with NS, the effect of LTG (approach I) and of LOV (approach II) is investigated on synaptic plasticity and alertness. LTG is tested in patients with NF1 (approach III). Trial participants receive a single dose of 300 mg LTG or placebo (I and III) and 200 mg LOV or placebo (II) daily for 4 days with a cross-over after at least 7 days. Synaptic plasticity is investigated using a repetitive high-frequency transcranial magnetic stimulation (TMS) protocol called quadri-pulse theta burst stimulation (qTBS). Attention is examined by using the test of attentional performance (TAP). Twenty-eight patients are randomized in groups NS and NF1 with n = 24 intended to reach the primary endpoint (change in synaptic plasticity). Secondary endpoints are attention (TAP) and differences in short interval cortical inhibition (SICI) between placebo and trial medication (LTG and LOV).
Discussion: The study is targeting impairments in synaptic plasticity and cognitive impairment, one of the main health problems of patients with RASopathies. Recent first results with LOV in patients with NF1 have shown an improvement in synaptic plasticity and cognition. Within this clinical trial, it is investigated if these findings can be transferred to patients with NS. LTG is most likely a more effective and promising substance improving synaptic plasticity and, consecutively, cognitive function. It is expected that both substances are improving synaptic plasticity as well as alertness. Changes in alertness may be a precondition for improvement of cognition.
Trial registration: The clinical trial is registered in ClinicalTrials.gov (NCT03504501; https://www.
Clinicaltrials: gov ; date of registration: 04/11/2018) and in EudraCT (number 2016-005022-10).
Keywords: Attention; Lamotrigine; Lovastatin; Neurofibromatosis type 1; Noonan syndrome; RASopathies; Synaptic plasticity; Transcranial magnetic stimulation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
