

Neuropathology of the Alzheimer's continuum: an update
- PMID: 37283686
- PMCID: PMC10209886
- DOI: 10.17879/freeneuropathology-2020-3050
Neuropathology of the Alzheimer's continuum: an update
Abstract
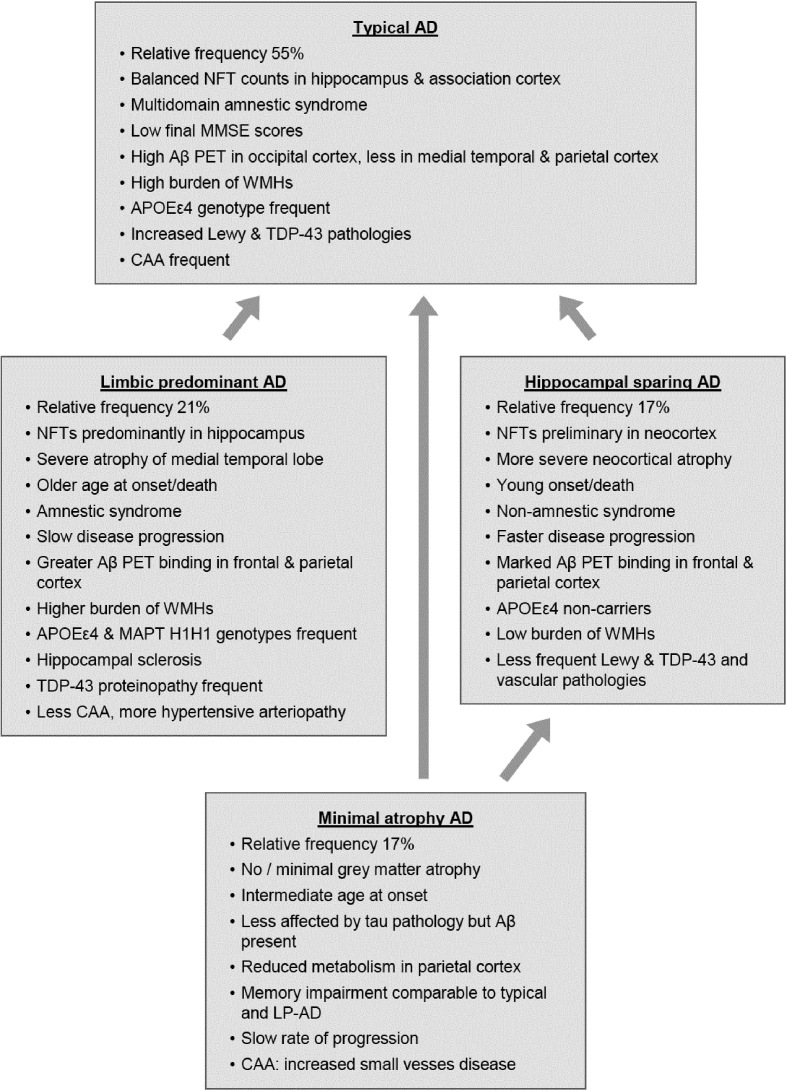
Alzheimer's disease (AD), the most common form of dementia worldwide, is a mixed proteinopathy (amyloid and tau). Originally defined as a clinicopathological entity, it is a heterogenous, multifactorial disorder, currently referred to as the Alzheimer's continuum. Its cardinal pathological features are extracellular β-amyloid (amyloid plaques) and intraneuronal tau aggregates forming neurofibrillary tangles, which are accompanied by vascular amyloid deposits (cerebral amyloid angiopathy), synapse and neuronal loss, as well as neuroinflammation and reactive astrogliosis. In addition to "typical" AD, various subtypes with characteristic regional patterns of tau pathology have been described that show distinct clinical features, biomarker levels, and patterns of key network destructions responsible for cognitive decline. AD is frequently associated with other age-related changes including Lewy and TDP-43 pathologies, hippocampal sclerosis, argyrophilic grain disease, cerebrovascular lesions, and others. These additional pathologies influence the clinical picture of AD, may accelerate disease progression, and can cause a number of challenges in our understanding of the disease including the threshold of each individual pathology to cause dementia and the possibility of underlying common etiologies. This article provides an up-to-date overview of AD neuropathology, its heterogeneity, and additional pathologies in order to explain the difficulties in the diagnosis and the failure of clinical trials in AD patients.
Keywords: Alzheimer subtypes; Alzheimer’s disease; Amyloid angiopathy; Co-pathologies; Oligomers; Regional vulnerabiliy; Tau pathology; β-Amyloid.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
-
- Alzheimer's-Association (2018) 2018 Alzheimer's disease facts and figures. Alzheimers Dement 14:367-429
-
- Jellinger KA, Attems J (2010) Prevalence of dementia disorders in the oldest-old: an autopsy study. Acta Neuropathol 119:421-433 - PubMed
-
- Fiest KM, Roberts JI, Maxwell CJ, Hogan DB, Smith EE, Frolkis A, Cohen A, Kirk A, Pearson D, Pringsheim T, Venegas-Torres A, Jetté N (2016) The prevalence and incidence of dementia due to Alzheimer's disease: a systematic review and meta-analysis. Canad J Neurol Sci 43 (Suppl S1):S51-S82 - PubMed
LinkOut - more resources
Full Text Sources