

The Metastatic Risk of Renal Cell Carcinoma by Primary Tumor Size and Subtype
- PMID: 37284045
- PMCID: PMC10240521
- DOI: 10.1016/j.euros.2023.04.015
The Metastatic Risk of Renal Cell Carcinoma by Primary Tumor Size and Subtype
Abstract
Background: Current data on the association between tumor size, subtype, and metastases, and thresholds for intervention, for renal cell carcinoma (RCC), are largely based on single-center nephrectomy registries that may under-represent those presenting with metastatic disease.
Objective: We sought to assess tumor size and histologic subtype in relation to metastatic status at presentation for patients with RCC.
Design setting and participants: Using Surveillance, Epidemiology and End Results cancer registry data, we identified patients with a diagnosis of RCC made between 2004 and 2019, and a known size of primary tumor. We used nodal and metastatic TNM staging to assess metastatic disease at presentation.
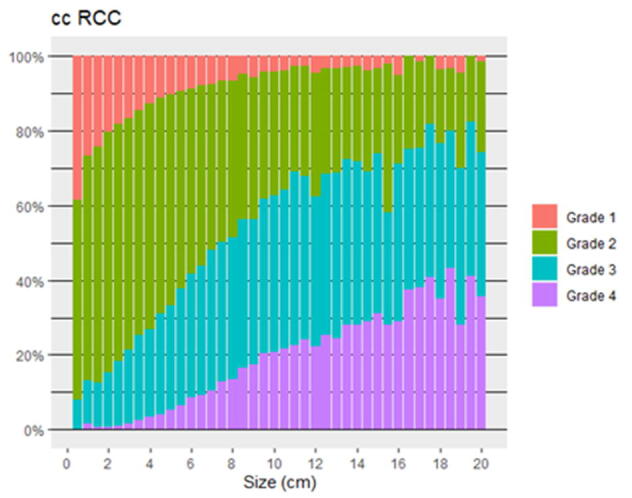
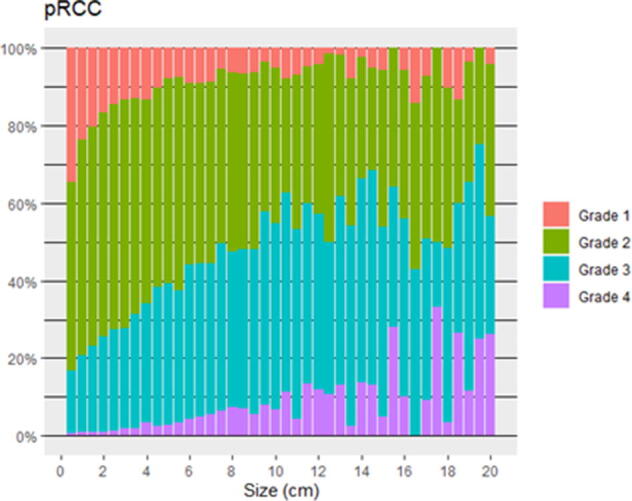
Outcome measurements and statistical analysis: We report the proportion of metastatic disease across varying tumor sizes for clear cell (ccRCC), papillary (pRCC), and chromophobe (chRCC) RCC. We also examine sarcomatoid RCC and RCC with sarcomatoid features (sarcRCC). Logistic regression models were used to model the likelihood of metastatic disease for each histologic subtype.
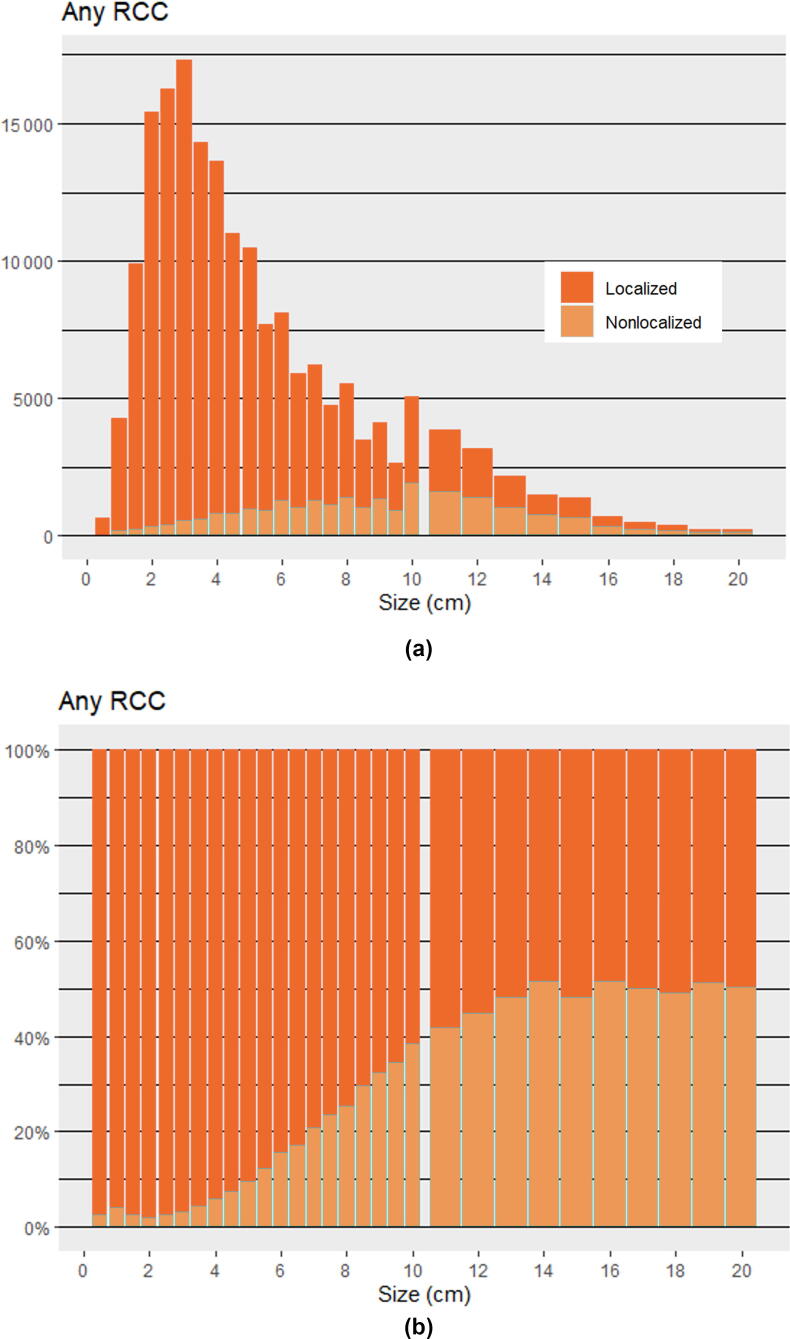
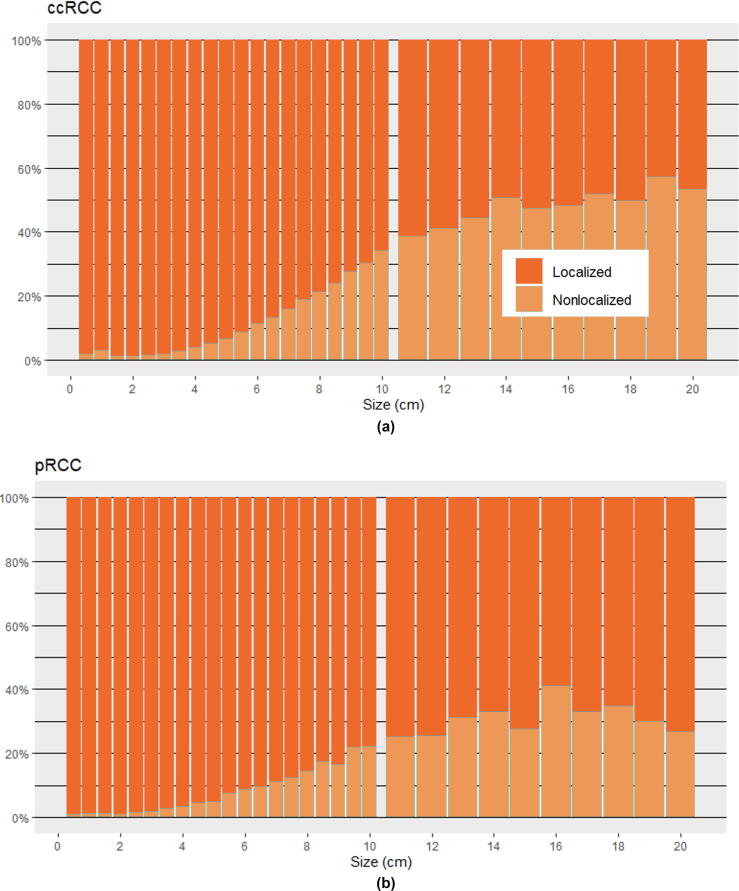
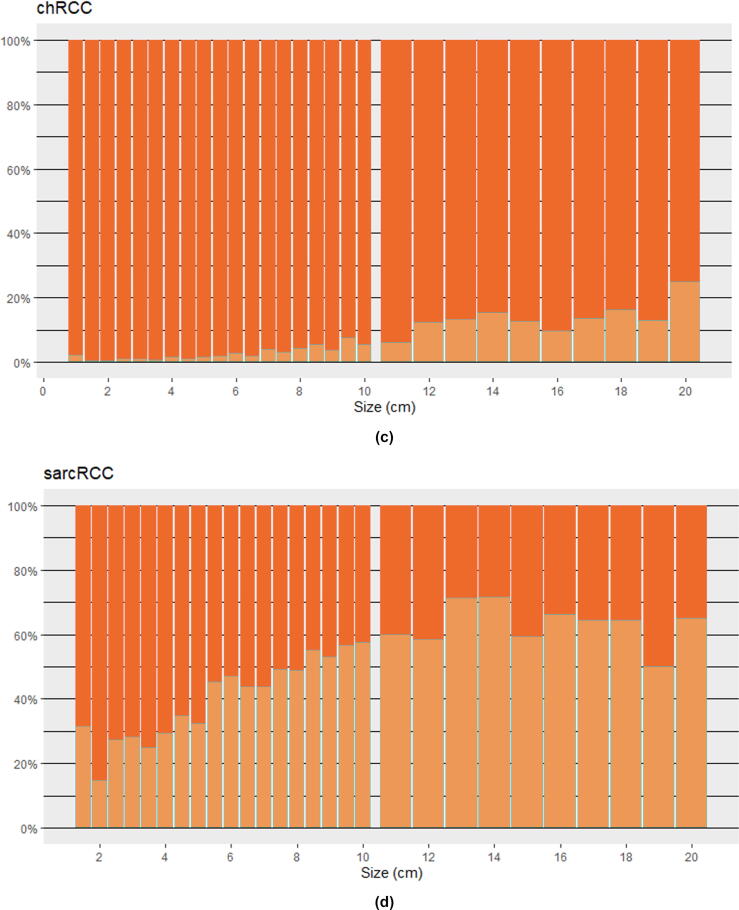
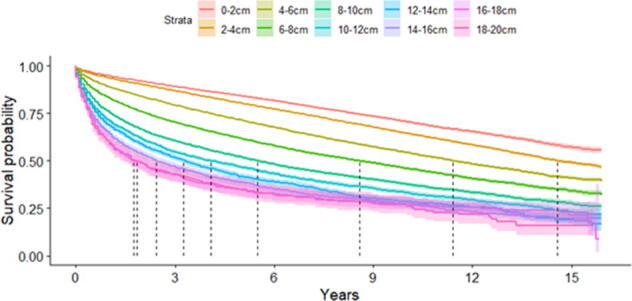
Results and limitations: Of 181 096 RCC patients included, 23 829 had metastatic disease. For any RCC, metastatic rates of 3.6%, 13.1%, 30.3%, and 45.1% were observed for tumors ≤4, 4-≤7, 7-≤10, and >10 cm, respectively. Metastatic rates of chRCC were low at even large sizes, 11.0% at >10 cm. In contrast, sarcRCC had high metastatic rates at all sizes, 27.1% at ≤4 cm. Metastatic rates for ccRCC and pRCC increased steadily above 3 cm. For any RCC and each evaluated subtype, tumor size was found to be associated with metastatic disease on logistic regression (p < 0.001).
Conclusions: The likelihood of a renal mass being metastatic varies greatly with both its subtype and size. We report higher likelihoods of metastatic disease across tumor sizes compared with what has been reported previously. These results may help clinicians pick appropriate thresholds for intervention and candidates for active surveillance.
Patient summary: We find that the metastatic probability of renal cell carcinoma varies greatly with subtype and increases with tumor size.
Keywords: Active surveillance; Epidemiology and End Results; Histology; Renal cell carcinoma; Renal mass biopsy; Surveillance.
© 2023 The Authors.
Figures
References
-
- Capitanio U., Montorsi F. Renal cancer. Lancet. 2016;387:894–906. - PubMed
-
- Sharp E., Guduru A., May A.M., Lombardo L., Siddiqui S.A., Hamilton Z.A. The distribution of metastatic renal cell carcinoma by presenting tumor stage in the modern era. Clin Genitourin Cancer. 2022;20:e296–e302. - PubMed
-
- McIntosh A.G., Ristau B.T., Ruth K., et al. Active surveillance for localized renal masses: tumor growth, delayed intervention rates, and >5-yr clinical outcomes. Eur Urol. 2018;74:157–164. - PubMed
-
- EAU. Guidelines. Presented at the EAU Annual Congress Amsterdam; 2022. https://uroweb.org/guidelines/renal-cell-carcinoma.
