

Local Control Failure After Five-Fraction Stereotactic Radiosurgery Alone for Symptomatic Brain Metastasis From Squamous Cell Lung Carcinoma Despite 43 Gy to Gross Tumor Margin With Internal Steep Dose Increase and Tumor Shrinkage During Irradiation
- PMID: 37284398
- PMCID: PMC10241550
- DOI: 10.7759/cureus.38645
Local Control Failure After Five-Fraction Stereotactic Radiosurgery Alone for Symptomatic Brain Metastasis From Squamous Cell Lung Carcinoma Despite 43 Gy to Gross Tumor Margin With Internal Steep Dose Increase and Tumor Shrinkage During Irradiation
Abstract
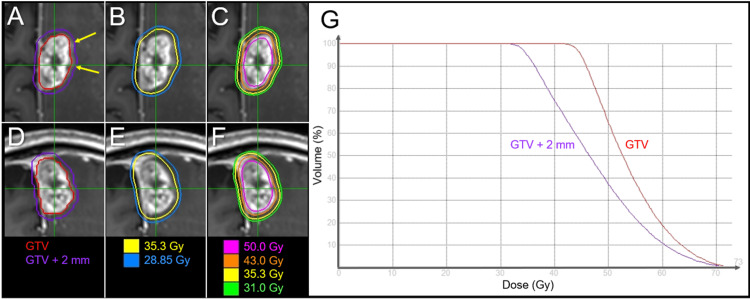
Five-fraction (fr) stereotactic radiosurgery (SRS) is increasingly being applied to large brain metastases (BMs) >2-3 cm in diameter, for which 30-35 Gy is the commonly prescribed dose. Since 2018, to further enhance both safety and efficacy, we have limited the five-fr SRS to approximately ≤3 cm BMs and adopted our own modified dose prescription and distribution: 43 and 31 Gy cover the boundaries of the gross tumor volume (GTV) and 2 mm outside the GTV, respectively, along with a steep dose increase inside the GTV boundary, that is, an intentionally very inhomogeneous GTV dose. Herein, we describe a case of symptomatic BM treated with five-fr SRS using the above policy, which resulted in a maximum tumor response with nearly complete remission (nCR) followed by gradual tumor regrowth despite obvious tumor shrinkage during irradiation. A 71-year-old man who had previously undergone surgery for squamous cell carcinoma (SCC) of the lungs presented with right-sided hemiparesis attributed to the para-falcine BM (27 mm in maximum diameter, 5.38 cm3). The BM was treated with five-fr SRS, with 99.2% of the GTV covered with 43 Gy and 59% isodose. Neurological symptoms improved during SRS, and obvious tumor shrinkage and mitigation of perilesional edema were observed upon completion of SRS. No subsequent anti-cancer pharmacotherapy was administered due to idiopathic pulmonary fibrosis (IPF). Despite a maximum response with nCR at four months, the tiny residual enhancing lesion gradually enlarged from 7.7 months to 22.7 months without neurological worsening. Although a consistent T1/T2 mismatch suggested the dominance of brain radionecrosis, 11C-methionine positron emission tomography showed increased uptake in the enhancing lesion. Pathological examination after total lesionectomy at 24.6 months revealed viable tumor tissue. Post-SRS administration of nintedanib for IPF may have provided some anti-tumor efficacy for lung SCC and may mitigate the adverse effects of SRS. The present case suggests that even ≥43 Gy with ≤60% isodose to the GTV boundary and ≥31-35 Gy to the 2 mm outside the GTV are insufficient to achieve long-term local tumor control by five-fr SRS alone in some large BM from lung SCC.
Keywords: biological effective dose; brain metastasis; five fraction; fractionation; linear-quadratic model; lung cancer; neuroendoscopy; nintedanib; squamous cell carcinoma; stereotactic radiosurgery.
Copyright © 2023, Ohtakara et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- Tumor control probability of radiosurgery and fractionated stereotactic radiosurgery for brain metastases. Redmond KJ, Gui C, Benedict S, et al. Int J Radiat Oncol Biol Phys. 2021;110:53–67. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials