

Comparison of different adjuvant therapy regimen efficacies in patients with high risk of recurrence after radical resection of hepatocellular carcinoma
- PMID: 37284841
- PMCID: PMC11797173
- DOI: 10.1007/s00432-023-04874-0
Comparison of different adjuvant therapy regimen efficacies in patients with high risk of recurrence after radical resection of hepatocellular carcinoma
Abstract
Background: Hepatocellular carcinoma (HCC) has a high recurrence rate even after radical surgery. Postoperative adjuvant transhepatic arterial chemoembolization (PA-TACE), postoperative adjuvant hepatic arterial infusion chemotherapy (PA-HAIC), postoperative adjuvant radiotherapy (PA-RT), and postoperative adjuvant molecular targeted therapy have been demonstrated to be effective in reducing the postoperative recurrence rate. The present network meta-analysis was conducted to compare the effects of PA-TACE, PA-HAIC, PA-RT and postoperative adjuvant molecular targeted therapy on the overall survival (OS) and disease-free survival (DFS) in HCC patients after radical resection and to determine the optimal treatment strategy.
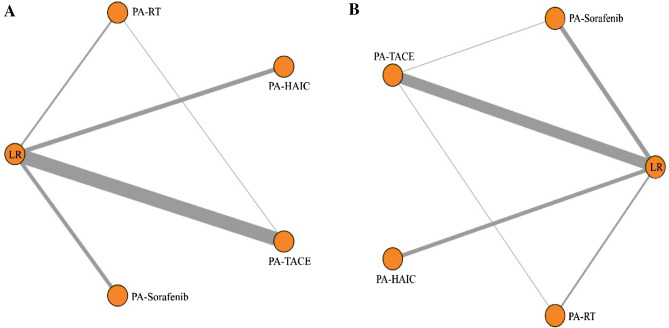
Methods: Network meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. PubMed, Embase, Cochrane Library, and Web of Science were used to collect eligible studies up to December 25, 2022. Studies related to PA-TACE, PA-HAIC, and postoperative adjuvant molecular targeted therapy after radical HCC resection was included. The endpoints were OS and DFS, and the effect size was determined using hazard ratio with a 95% confidence interval. R software and "gemtc" package were employed to analyze the results.
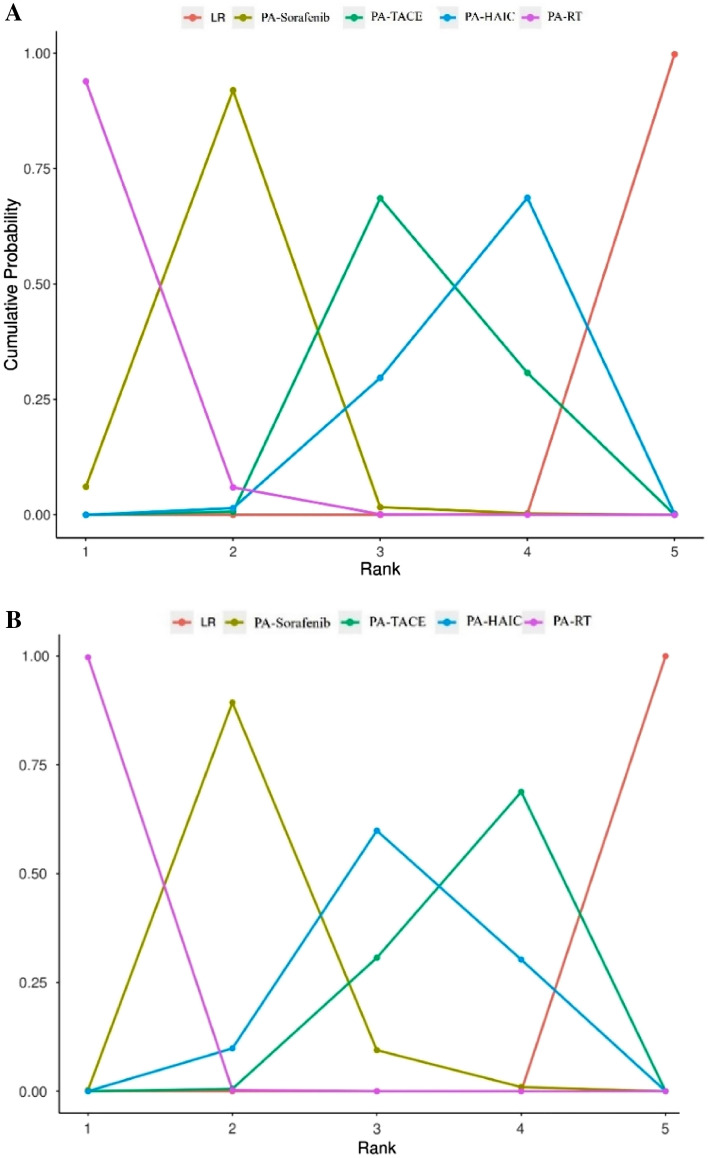
Results: A total of 38 studies involving 7079 patients with HCC after radical resection were ultimately enrolled to be analyzed. Four postoperative adjuvant therapy measures and two oncology indicators were evaluated. In this study, OS-related investigations validated that PA-Sorafenib and PA-RT markedly enhanced the OS rates in patients after radical resection when compared to PA-TACE and PA-HAIC. However, statistical analysis revealed no significant difference between PA-Sorafenib and PA-RT, as well as PA-TACE and PA-HAIC. In the DFS-related investigations, PA-RT demonstrated superior efficacy over PA-Sorafenib, PA-TACE, and PA-HAIC. Additionally, PA-Sorafenib displayed better efficacy than PA-TACE. Nevertheless, there was no statistical significance between PA-Sorafenib and PA-HAIC, as well as PA-TACE and PA-HAIC. We also performed a subgroup analysis of studies focusing on HCC complicated by microvascular invasion after radical resection. In terms of OS, both PA-RT and PA-Sorafenib demonstrated a noteworthy improvement over PA-TACE, whereas no statistical significance was detected between PA-RT and PA-Sorafenib. Likewise, for DFS, both PA-Sorafenib and PA-RT exhibited superior efficacy compared to PA-TACE.
Conclusion: In patients with HCC after radical resection and a high risk of recurrence, both PA-Sorafenib and PA-RT significantly improved OS and DFS when compared to PA-TACE and PA-HAIC. Notably, PA-RT exhibited superior efficacy over PA-Sorafenib, PA-TACE, and PA-HAIC in terms of DFS. Similarly, PA-Sorafenib appeared to be more effective than PA-TACE for DFS.
Keywords: Adjuvant therapy; Hepatectomy; Hepatocellular carcinoma; Network meta-analysis.
© 2023. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures




References
-
- Benson AB et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Comprehensive Cancer Netw 19: 541–565, 10.6004/jnccn.2021.0022 (2021). - PubMed
-
- Berg TJ, Pietras A (2022) Radiotherapy-induced remodeling of the tumor microenvironment by stromal cells. Semin Cancer Biol 86:846–856. 10.1016/j.semcancer.2022.02.011 - PubMed
-
- Chen ZH et al (2019) Adjuvant transarterial chemoembolization improves survival outcomes in hepatocellular carcinoma with microvascular invasion: a systematic review and meta-analysis. Eur J Surg Oncol 45:2188–2196. 10.1016/j.ejso.2019.06.031 - PubMed
-
- Chen W et al (2020) A systematic review and meta-analysis of adjuvant transarterial chemoembolization after curative resection for patients with hepatocellular carcinoma. HPB (oxford) 22:795–808. 10.1016/j.hpb.2019.12.013 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
