

Less Irradiation to Lymphocyte-Related Organs Reduced the Risk of G4 Lymphopenia in Esophageal Cancer: Re-Analysis of Prospective Trials
- PMID: 37285035
- PMCID: PMC10400141
- DOI: 10.1093/oncolo/oyad109
Less Irradiation to Lymphocyte-Related Organs Reduced the Risk of G4 Lymphopenia in Esophageal Cancer: Re-Analysis of Prospective Trials
Abstract
Background: This study aimed to explore the relationship between irradiation of lymphocyte-related organs at risk (LOARs) and lymphopenia during definitive concurrent chemoradiotherapy (dCCRT) for esophageal squamous cell carcinoma (ESCC).
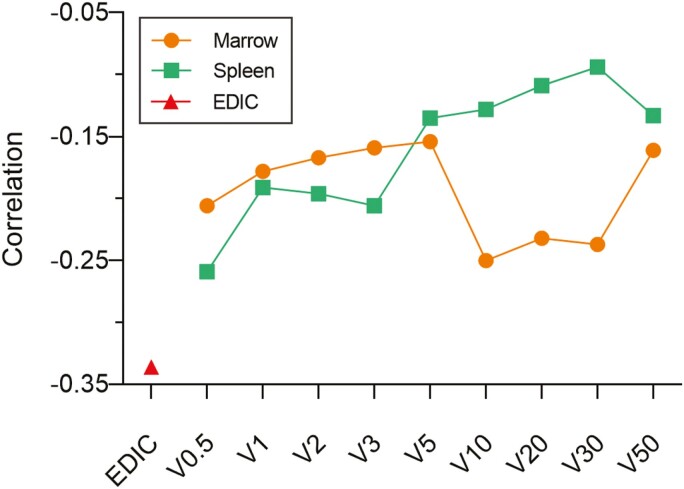
Materials and methods: Cases of ESCC patients who received dCCRT from 2 prospective clinical trials were identified. To find its correlation with survival outcomes, grades of absolute lymphocyte counts (ALCs) nadir during radiotherapy were recorded following COX analysis. Associations of lymphocytes at nadir and dosimetric parameters including relative volumes of spleen and bone marrow receiving 0.5, 1, 2, 3, 5, 10, 20, 30, and 50Gy (V0.5, V1, V2, V3, V5, V10, V20, V30, and V50), and effective dose to circulating immune cells (EDIC) were examined by logistic risk regression analysis. The cutoffs of dosimetric parameters were determined by the receiver operating characteristic curve (ROC).
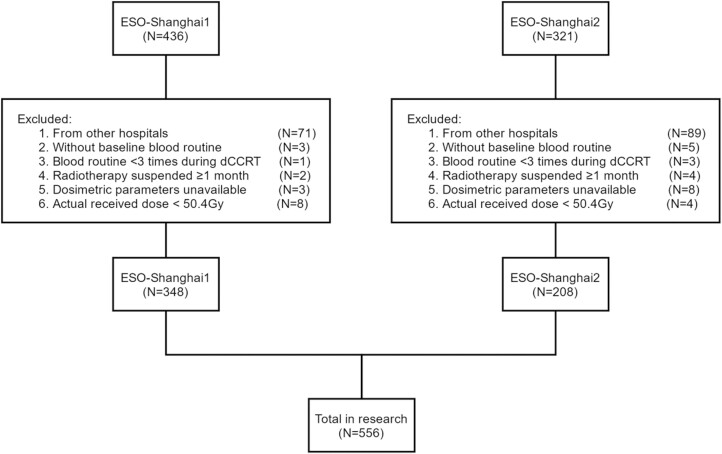
Results: A total of 556 patients were included. The incidences of grades 0, 1, 2, 3, and 4 (G4) lymphopenia during dCCRT were 0.2%, 0.5%, 9.7%, 59.7%, and 29.8%, respectively. Their median overall survival (OS) and progression-free survival (PFS) time were 50.2 and 24.3 months, respectively; the incidence of local recurrence and distant metastasis were 36.6% and 31.8%, respectively. Patients once suffering from G4 nadir during radiotherapy had unfavorable OS (HR, 1.28; P = .044) and a higher incidence of distant metastasis (HR, 1.52; P = .013). Furthermore, patients with EDIC ≤8.3Gy plus spleen V0.5 ≤11.1% and bone marrow V10 ≤33.2% were strongly associated with lower risk of G4 nadir (OR, 0.41; P = .004), better OS (HR, 0.71; P = .011) and lower risk of distant metastasis (HR, 0.56; P = .002).
Conclusions: Smaller relative volumes of spleen V0.5 and bone marrow V10 plus lower EDIC were jointly prone to reduce the incidence of G4 nadir during definitive concurrent chemoradiotherapy. This modified therapeutic strategy could be a significant prognostic factor for survival outcomes in ESCC.
Keywords: chemoradiotherapy; esophageal cancer; lymphocyte-related organs at risk.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
The authors indicated no financial relationships.
Figures


References
-
- Yovino S, Kleinberg L, Grossman SA, Narayanan M, Ford E.. The etiology of treatment-related lymphopenia in patients with malignant gliomas: modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Invest. 2013;31(2):140-144. 10.3109/07357907.2012.762780. - DOI - PMC - PubMed
-
- Lambin P, Lieverse R, Eckert F, et al. . Lymphocyte-sparing radiotherapy: the rationale for protecting lymphocyte-rich organs when combining radiotherapy with immunotherapy. Semin Radiat Oncol. 2020;30(2):187-193. https://doi.org/10.1016/j.semradonc.2019.12.003. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
