

Safety of Targeted Axillary Dissection After Neoadjuvant Therapy in Patients With Node-Positive Breast Cancer
- PMID: 37285140
- PMCID: PMC10248815
- DOI: 10.1001/jamasurg.2023.1772
Safety of Targeted Axillary Dissection After Neoadjuvant Therapy in Patients With Node-Positive Breast Cancer
Abstract
Importance: The increasing use of neoadjuvant systemic therapy (NST) has led to substantial pathological complete response rates in patients with initially node-positive, early breast cancer, thereby questioning the need for axillary lymph node dissection (ALND). Targeted axillary dissection (TAD) is feasible for axillary staging; however, data on oncological safety are scarce.
Objective: To assess 3-year clinical outcomes in patients with node-positive breast cancer who underwent TAD alone or TAD with ALND.
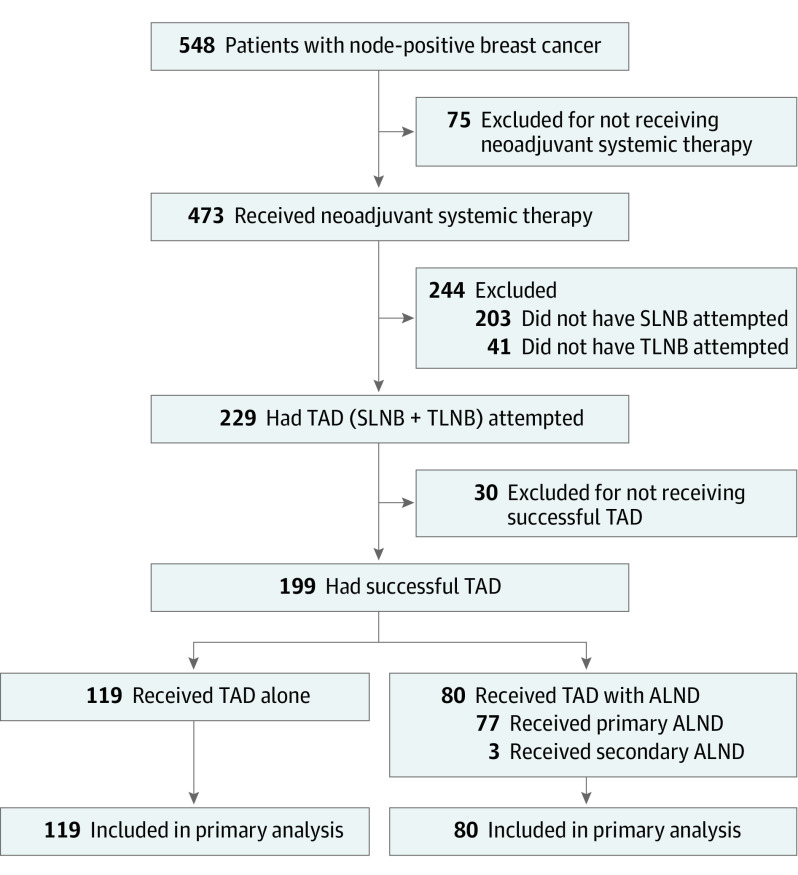
Design, setting, and participants: The SenTa study is a prospective registry study and was conducted between January 2017 and October 2018. The registry includes 50 study centers in Germany. Patients with clinically node-positive breast cancer underwent clipping of the most suspicious lymph node (LN) before NST. After NST, the marked LNs and sentinel LNs were excised (TAD) followed by ALND according to the clinician's choice. Patients who did not undergo TAD were excluded. Data analysis was performed in April 2022 after 43 months of follow-up.
Exposure: TAD alone vs TAD with ALND.
Main outcomes and measures: Three-year clinical outcomes were evaluated.
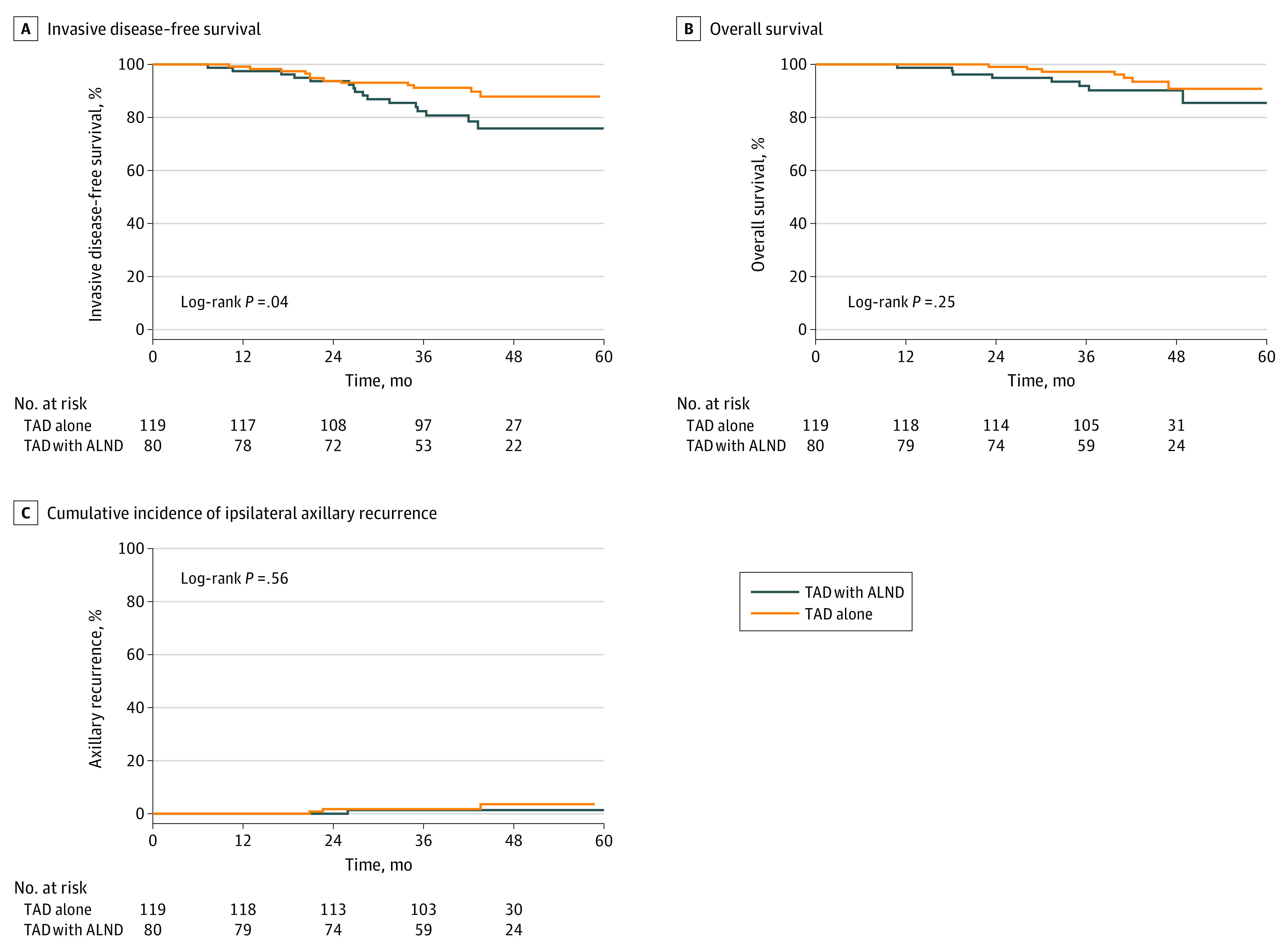
Results: Of 199 female patients, the median (IQR) age was 52 (45-60) years. A total of 182 patients (91.5%) had 1 to 3 suspicious LNs; 119 received TAD alone and 80 received TAD with ALND. Unadjusted invasive disease-free survival was 82.4% (95% CI, 71.5-89.4) in the TAD with ALND group and 91.2% (95% CI, 84.2-95.1) in the TAD alone group (P = .04); axillary recurrence rates were 1.4% (95% CI, 0-54.8) and 1.8% (95% CI, 0-36.4), respectively (P = .56). Adjusted multivariate Cox regression indicated that TAD alone was not associated with an increased risk of recurrence (hazard ratio [HR], 0.83; 95% CI, 0.34-2.05; P = .69) or death (HR, 1.07; 95% CI, 0.31-3.70; P = .91). Similar results were obtained for 152 patients with clinically node-negative breast cancer after NST (invasive disease-free survival: HR, 1.26; 95% CI, 0.27-5.87; P = .77; overall survival: HR, 0.81; 95% CI, 0.15-3.83; P = .74).
Conclusions and relevance: These results suggest that TAD alone in patients with mostly good clinical response to NST and at least 3 TAD LNs may confer survival outcomes and recurrence rates similar to TAD with ALND.
Conflict of interest statement
Figures
Comment in
-
Evidence-Based De-Escalation in Axillary Management-Is Less Really More?JAMA Surg. 2023 Aug 1;158(8):816. doi: 10.1001/jamasurg.2023.1783. JAMA Surg. 2023. PMID: 37285138 Free PMC article. No abstract available.
References
-
- Loibl S, Jackisch C, Schneeweiss A, et al. ; investigators of the German Breast Group (GBG) and the Arbeitsgemeinschaft Gynäkologische Onkologie—Breast (AGO-B) study groups . Dual HER2-blockade with pertuzumab and trastuzumab in HER2-positive early breast cancer: a subanalysis of data from the randomized phase III GeparSepto trial. Ann Oncol. 2017;28(3):497-504. doi:10.1093/annonc/mdw610 - DOI - PubMed
-
- Hurvitz SA, Martin M, Symmans WF, et al. . Neoadjuvant trastuzumab, pertuzumab, and chemotherapy versus trastuzumab emtansine plus pertuzumab in patients with HER2-positive breast cancer (KRISTINE): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2018;19(1):115-126. doi:10.1016/S1470-2045(17)30716-7 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
