

Inflammation, lipids, and pain in vulvar disease
- PMID: 37285943
- PMCID: PMC10527276
- DOI: 10.1016/j.pharmthera.2023.108467
Inflammation, lipids, and pain in vulvar disease
Abstract
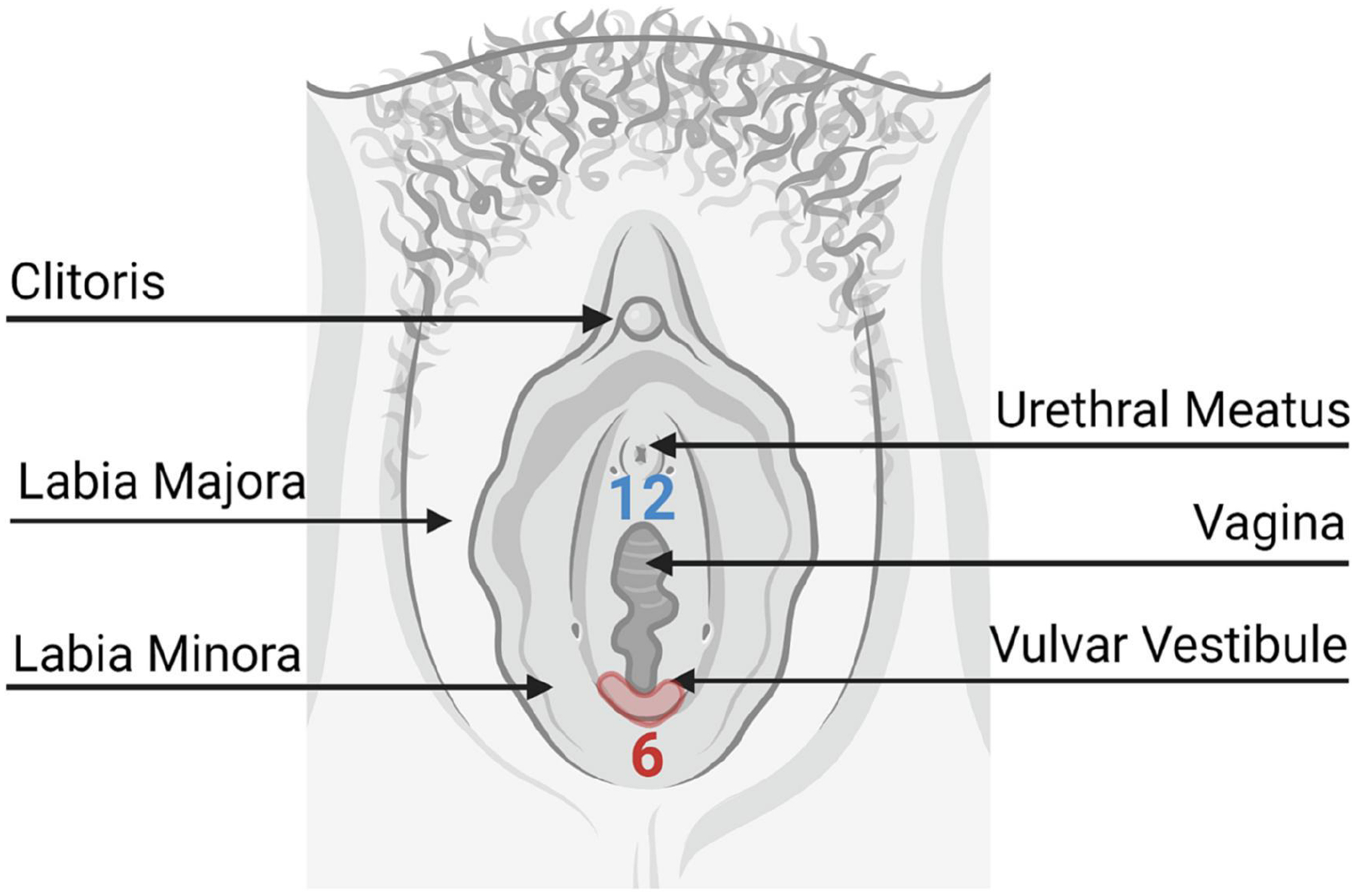
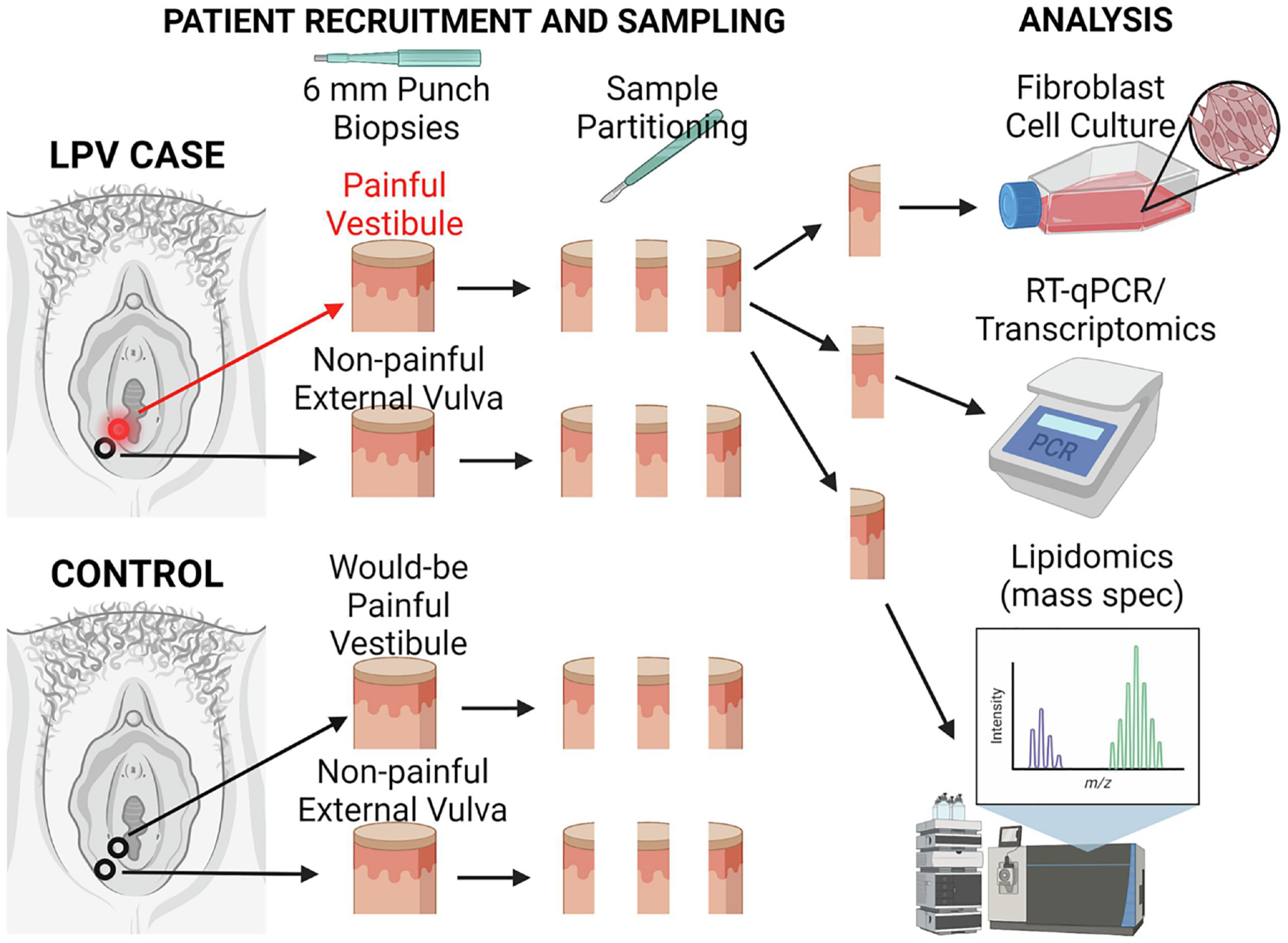
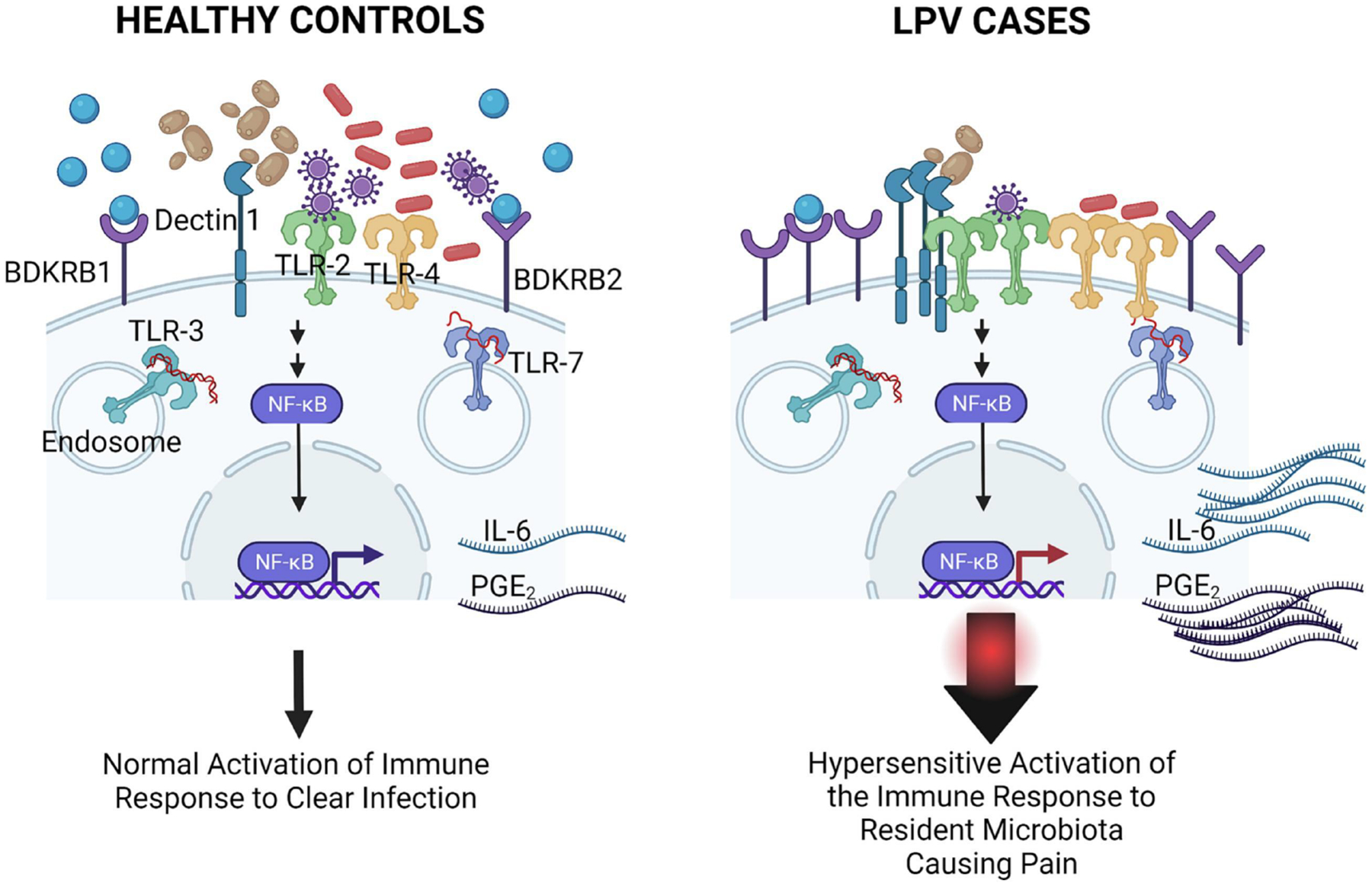
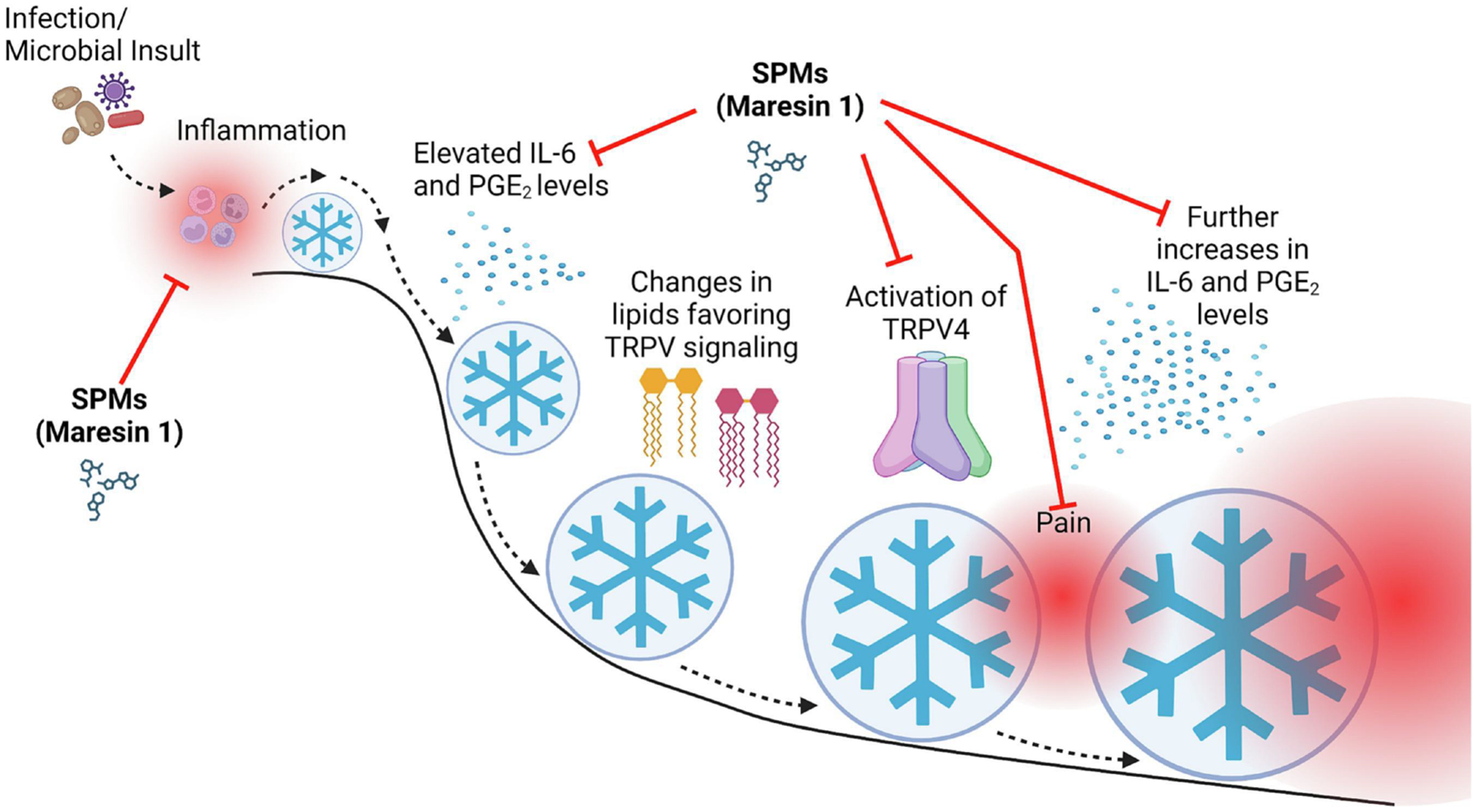
Localized provoked vulvodynia (LPV) affects ∼14 million people in the US (9% of women), destroying lives and relationships. LPV is characterized by chronic pain (>3 months) upon touch to the vulvar vestibule, which surrounds the vaginal opening. Many patients go months or years without a diagnosis. Once diagnosed, the treatments available only manage the symptoms of disease and do not correct the underlying problem. We have focused on elucidating the underlying mechanisms of chronic vulvar pain to speed diagnosis and improve intervention and management. We determined the inflammatory response to microorganisms, even members of the resident microflora, sets off a chain of events that culminates in chronic pain. This agrees with findings from several other groups, which show inflammation is altered in the painful vestibule. The vestibule of patients is acutely sensitive to inflammatory stimuli to the point of being deleterious. Rather than protect against vaginal infection, it causes heightened inflammation that does not resolve, which coincides with alterations in lipid metabolism that favor production of proinflammatory lipids and not pro-resolving lipids. Lipid dysbiosis in turn triggers pain signaling through the transient receptor potential vanilloid subtype 4 receptor (TRPV4). Treatment with specialized pro-resolving mediators (SPMs) that foster resolution reduces inflammation in fibroblasts and mice and vulvar sensitivity in mice. SPMs, specifically maresin 1, act on more than one part of the vulvodynia mechanism by limiting inflammation and acutely inhibiting TRPV4 signaling. Therefore, SPMs or other agents that target inflammation and/or TRPV4 signaling could prove effective as new vulvodynia therapies.
Keywords: Fibroblasts; Inflammation; Lipids; Pain; SPMs; TRPV4; Vulvodynia.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest We do not have any conflicts of interest to disclose.
Figures
Similar articles
-
Specialized Pro-resolving Mediators Reduce Pro-nociceptive Inflammatory Mediator Production in Models of Localized Provoked Vulvodynia.J Pain. 2021 Oct;22(10):1195-1209. doi: 10.1016/j.jpain.2021.03.144. Epub 2021 Apr 1. J Pain. 2021. PMID: 33813057 Free PMC article.
-
Inflammation, lipid dysregulation, and transient receptor potential cation channel subfamily V member 4 signaling perpetuate chronic vulvar pain.Pain. 2024 Apr 1;165(4):820-837. doi: 10.1097/j.pain.0000000000003088. Epub 2023 Oct 26. Pain. 2024. PMID: 37889581 Free PMC article.
-
Toll-Like Receptor Signaling Contributes to Proinflammatory Mediator Production in Localized Provoked Vulvodynia.J Low Genit Tract Dis. 2018 Jan;22(1):52-57. doi: 10.1097/LGT.0000000000000364. J Low Genit Tract Dis. 2018. PMID: 29271858 Free PMC article.
-
Vulvodynia: The Role of Inflammation in the Etiology of Localized Provoked Pain of the Vulvar Vestibule (Vestibulodynia).Semin Reprod Med. 2015 Jul;33(4):239-45. doi: 10.1055/s-0035-1554919. Epub 2015 Jul 1. Semin Reprod Med. 2015. PMID: 26132928 Review.
-
A review of the available clinical therapies for vulvodynia management and new data implicating proinflammatory mediators in pain elicitation.BJOG. 2017 Jan;124(2):210-218. doi: 10.1111/1471-0528.14157. Epub 2016 Jun 17. BJOG. 2017. PMID: 27312009 Free PMC article. Review.
Cited by
-
The Connections Between Dietary Fatty Acids, Inflammation, and Chronic Disease.Nutrients. 2025 Jul 15;17(14):2322. doi: 10.3390/nu17142322. Nutrients. 2025. PMID: 40732947 Free PMC article.
-
The Involvement of Glutamate-mGluR5 Signaling in the Development of Vulvar Hypersensitivity.Int J Mol Sci. 2025 Jan 9;26(2):523. doi: 10.3390/ijms26020523. Int J Mol Sci. 2025. PMID: 39859236 Free PMC article.
-
Dysregulation of Arachidonic Acid Metabolism Drives Inflammatory Lipid Production in Localized Provoked Vulvodynia.Nutrients. 2025 Jul 5;17(13):2233. doi: 10.3390/nu17132233. Nutrients. 2025. PMID: 40647337 Free PMC article.
References
-
- Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, Coady D, consensus vulvar pain terminology committee of the International Society for the Study of Vulvovaginal D, International Society for the Study of Women’s Sexual H, International Pelvic Pain S. 2015 ISSVD, ISSWSH, and IPPS Consensus Terminology and Classification of Persistent Vulvar Pain and Vulvodynia. The journal of sexual medicine. 2016;13(4):607–12. Epub 2016/04/06. doi: 10.1016/j.jsxm.2016.02.167. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
