

Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of gastrointestinal cancer
- PMID: 37286304
- PMCID: PMC10254964
- DOI: 10.1136/jitc-2022-006658
Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of gastrointestinal cancer
Abstract
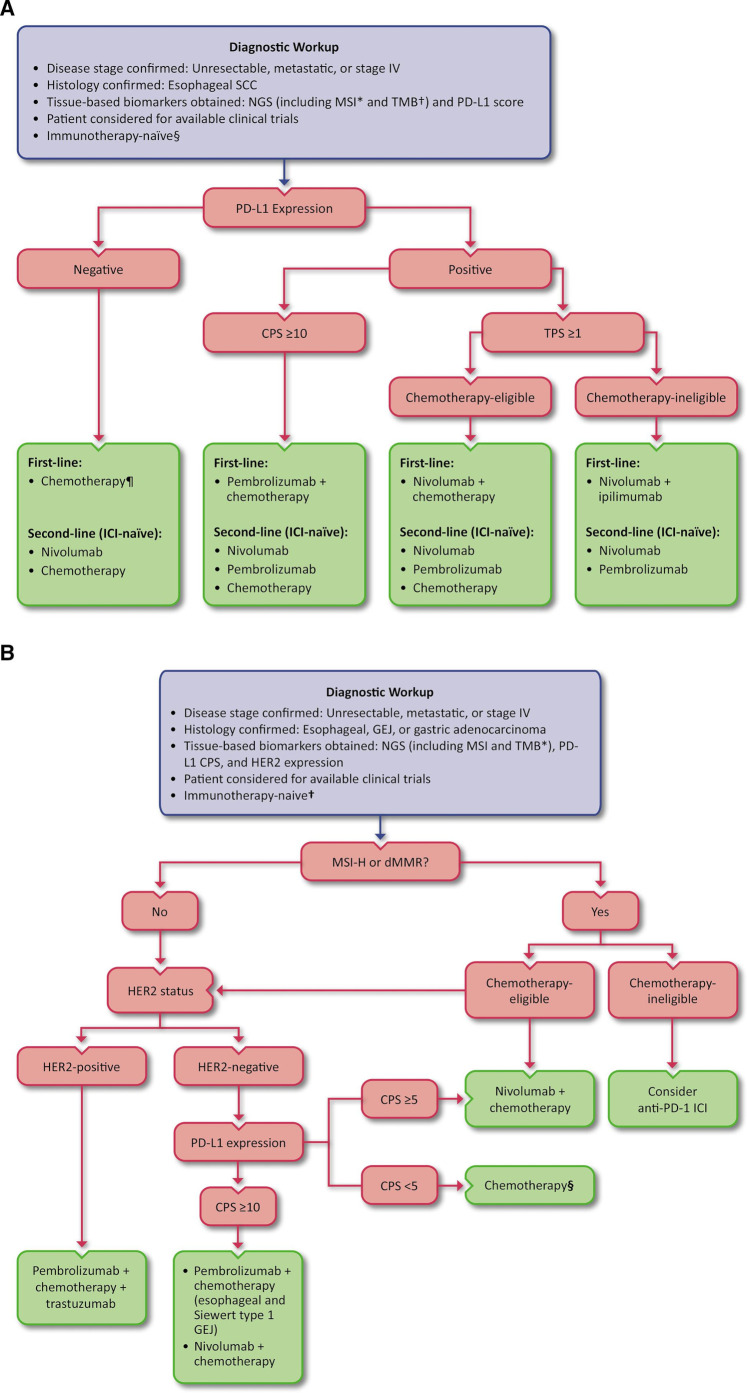
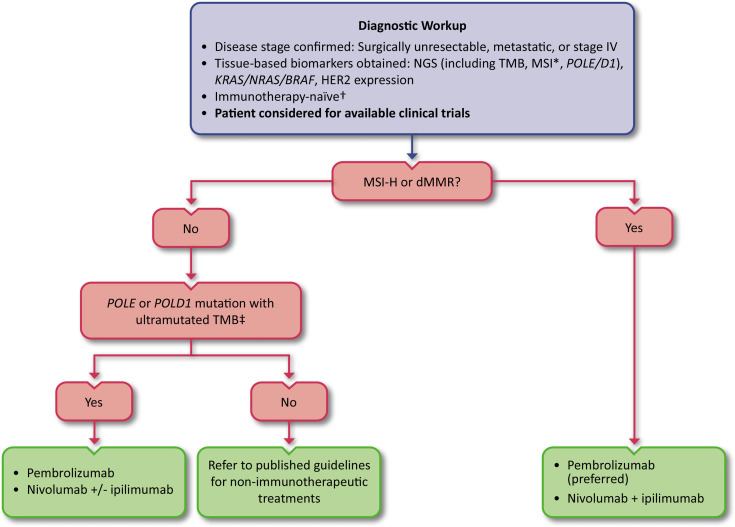
Gastrointestinal (GI) cancers, including esophageal, gastroesophageal junction, gastric, duodenal and distal small bowel, biliary tract, pancreatic, colon, rectal, and anal cancer, comprise a heterogeneous group of malignancies that impose a significant global burden. Immunotherapy has transformed the treatment landscape for several GI cancers, offering some patients durable responses and prolonged survival. Specifically, immune checkpoint inhibitors (ICIs) directed against programmed cell death protein 1 (PD-1), either as monotherapies or in combination regimens, have gained tissue site-specific regulatory approvals for the treatment of metastatic disease and in the resectable setting. Indications for ICIs in GI cancer, however, have differing biomarker and histology requirements depending on the anatomic site of origin. Furthermore, ICIs are associated with unique toxicity profiles compared with other systemic treatments that have long been the mainstay for GI cancer, such as chemotherapy. With the goal of improving patient care by providing guidance to the oncology community, the Society for Immunotherapy of Cancer (SITC) convened a panel of experts to develop this clinical practice guideline on immunotherapy for the treatment of GI cancer. Drawing from published data and clinical experience, the expert panel developed evidence- and consensus-based recommendations for healthcare professionals using ICIs to treat GI cancers, with topics including biomarker testing, therapy selection, and patient education and quality of life considerations, among others.
Keywords: gastrointestinal neoplasms; guidelines as topic.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KB—researcher: Bristol-Myers Squibb, Merck. JC—consulting fees: Lilly, Merck, AstraZeneca, Foundation Medicine, Daiichi Sankyo, Macrogenics, Amgen, Ono Pharmaceutical, Bristol-Myers Squibb, Astellas, Turning Point Therapeutics, Silverback Therapeutics, Novartis, Coherus Biosciences, Geneos, Roche; fees for non-CE services: Merck, Bristol-Myers Squibb; contracted research: Merck, Brooklyn Immunotherapeutics. KKC—consulting fees: Array, Natera, Merck, Pfizer, Lilly/Loxo; contracted research: BMS, Array, Incyte, Daiichi Sankyo, Nucana, AbbVie, Merck, Pfizer/Calithera (all funds to institution). CE—consulting fees: Boston Scientific, SK, Halio Dx, J&J, Merck, Natera; contracted research: Hutchinson, Merck, Elevar, Janssen. MF—consulting fees: Amgen, Array, Bayer, fSK, HalioDx, Mirati, Pfizer, Seattle Genetics, Taiho, Zhuhai Yufan Biotech; fees for non-CE services: Guardant360, Amgen; other: Amgen, AstraZenenca, Novartis, Bristol-Myers Squibb (grants to institution). LG—consulting fees: Agios, Debiopharm, Taiho, Alentis, Incyte, Klus, Pieris, QED, SIRTEX, AstraZeneca, H3Biomedicine. JH—consulting fees: Merck, Bayer, BeiGene; contracted research: Merck, Boston Biomedical, Treos Bio, Senhwa Pharmaceuticals, Bayer, Incyte, TriOncology, Seattle Genetics, Hutchison MediPharma, Pionyr Immunotherapeutics, Trovogene, G1 Therapeutics. RI—consulting fees: Ipsen, AstraZeneca, Teresa, Hexal AG, Incyte; contracted research: Ipsen, Tersera, Merck, Aveo. RJK—researcher: Bristol-Myers Squibb and Eli Lilly with institutional grants for investigator-initiated trials awarded to Johns Hopkins and Baylor University Medical Center; consultant advisor speaker: Bristol-Myers Squibb, Ono Pharmaceuticals, Merck, AstraZeneca, Daicchi Sankyo, Astellas, Eisai, Ipsen, Pieris, Novartis, Takeda, EMD Serono, Novocure, Grail, Toray, Eli Lilly. SK—contracted research: Bristol-Myers Squibb, Aravive, Pfizer. GK—consulting fees: Apexigen, AstraZeneca, BMS, Eli Lilly, Merck, Pieris, Zymeworks; contracted research: Arog, AstraZeneca, BMS, Daiichi Sankyo, Merck, Oncolys, Pieris, Zymeworks. DTL—consulting fees: Merck, Bristol-Myers Squibb, Janssen, Nouscom; contracted research: Merck, Bristol-Myers Squibb, Aduro Biotech, Medivir, Curegenix, Nouscom; other: Merck. VKM II—consulting fees: Bicara, Servier; contracted research: Pfizer, Bristol-Myers Squibb, EMD Serono, BioNTech, Novartis. ASP—consulting fees: Helsinn, BMS, Advanced Accelerator Applications, Hutchinson, Ipsen, Incyte, Exelixis, Pfizer, QED, Lilly, Mirati, Amgen. MAS—consulting fees: Lilly Pharmaceutical; contracted research: Merck, Bristol-Myers Squibb, Oncolys Biopharma. SITC staff—CG, AK, NL, SM-W—nothing to disclose.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials