

PEOPLE (NTC03447678), a phase II trial to test pembrolizumab as first-line treatment in patients with advanced NSCLC with PD-L1 <50%: a multiomics analysis
- PMID: 37286305
- PMCID: PMC10254948
- DOI: 10.1136/jitc-2023-006833
PEOPLE (NTC03447678), a phase II trial to test pembrolizumab as first-line treatment in patients with advanced NSCLC with PD-L1 <50%: a multiomics analysis
Erratum in
-
Correction: PEOPLE (NTC03447678), a phase II trial to test pembrolizumab as first-line treatment in patients with advanced NSCLC with PD-L1 <50%: a multiomics analysis.J Immunother Cancer. 2024 Jan 11;12(1):e006833corr1. doi: 10.1136/jitc-2023-006833corr1. J Immunother Cancer. 2024. PMID: 38212129 Free PMC article. No abstract available.
Abstract
Background: Chemoimmunotherapy represents the standard of care for patients with advanced non-small cell lung cancer (NSCLC) and programmed death-ligand 1 (PD-L1) <50%. Although single-agent pembrolizumab has also demonstrated some activity in this setting, no reliable biomarkers yet exist for selecting patients likely to respond to single-agent immunotherapy. The main purpose of the study was to identify potential new biomarkers associated with progression-free-survival (PFS) within a multiomics analysis.
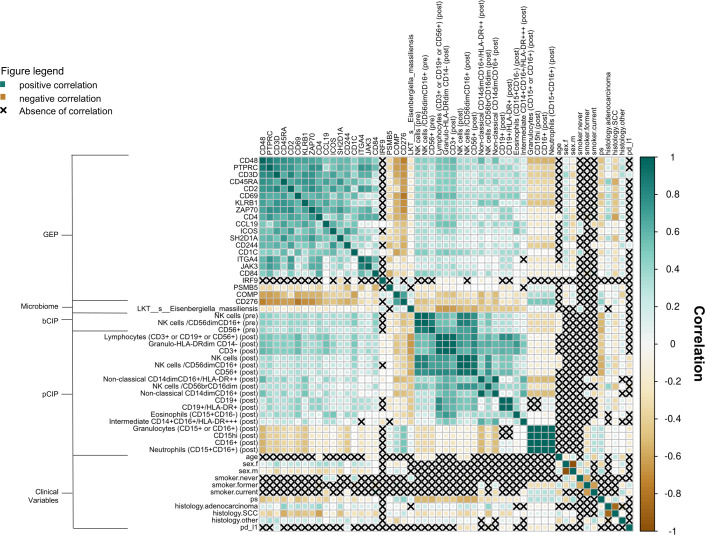
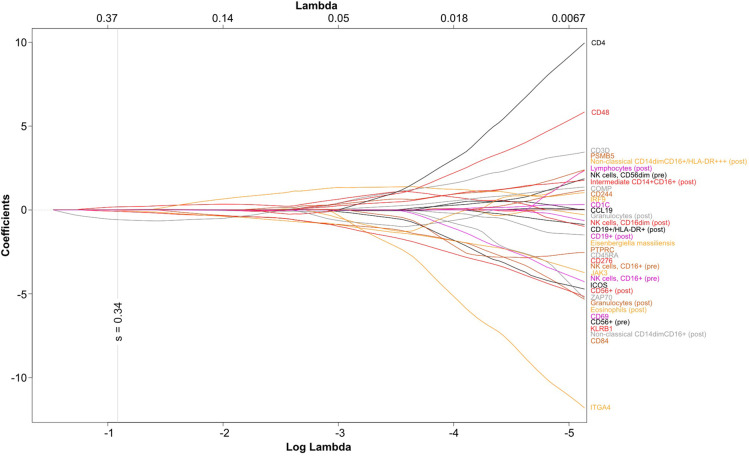
Methods: PEOPLE (NTC03447678) was a prospective phase II trial evaluating first-line pembrolizumab in patients with advanced EGFR and ALK wild type treatment-naïve NSCLC with PD-L1 <50%. Circulating immune profiling was performed by determination of absolute cell counts with multiparametric flow cytometry on freshly isolated whole blood samples at baseline and at first radiological evaluation. Gene expression profiling was performed using nCounter PanCancer IO 360 Panel (NanoString) on baseline tissue. Gut bacterial taxonomic abundance was obtained by shotgun metagenomic sequencing of stool samples at baseline. Omics data were analyzed with sequential univariate Cox proportional hazards regression predicting PFS, with Benjamini-Hochberg multiple comparisons correction. Biological features significant with univariate analysis were analyzed with multivariate least absolute shrinkage and selection operator (LASSO).
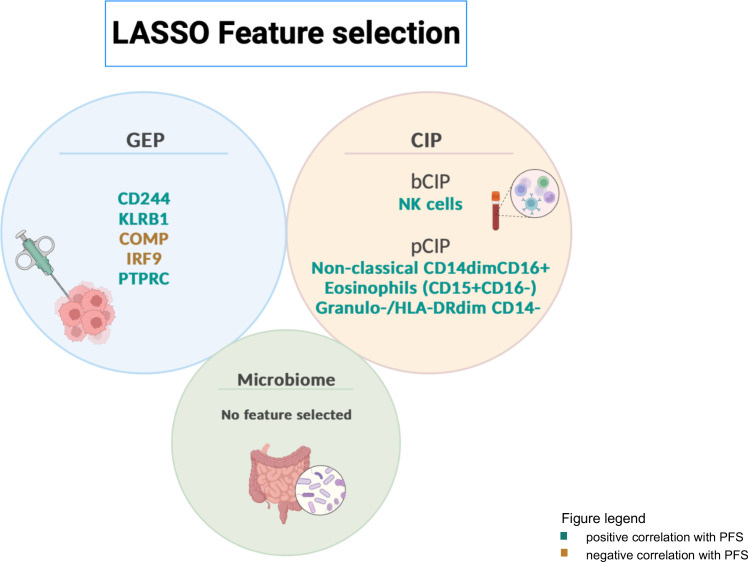
Results: From May 2018 to October 2020, 65 patients were enrolled. Median follow-up and PFS were 26.4 and 2.9 months, respectively. LASSO integration analysis, with an optimal lambda of 0.28, showed that peripheral blood natural killer cells/CD56dimCD16+ (HR 0.56, 0.41-0.76, p=0.006) abundance at baseline and non-classical CD14dimCD16+monocytes (HR 0.52, 0.36-0.75, p=0.004), eosinophils (CD15+CD16-) (HR 0.62, 0.44-0.89, p=0.03) and lymphocytes (HR 0.32, 0.19-0.56, p=0.001) after first radiologic evaluation correlated with favorable PFS as well as high baseline expression levels of CD244 (HR 0.74, 0.62-0.87, p=0.05) protein tyrosine phosphatase receptor type C (HR 0.55, 0.38-0.81, p=0.098) and killer cell lectin like receptor B1 (HR 0.76, 0.66-0.89, p=0.05). Interferon-responsive factor 9 and cartilage oligomeric matrix protein genes correlated with unfavorable PFS (HR 3.03, 1.52-6.02, p 0.08 and HR 1.22, 1.08-1.37, p=0.06, corrected). No microbiome features were selected.
Conclusions: This multiomics approach was able to identify immune cell subsets and expression levels of genes associated to PFS in patients with PD-L1 <50% NSCLC treated with first-line pembrolizumab. These preliminary data will be confirmed in the larger multicentric international I3LUNG trial (NCT05537922).
Trial registration number: 2017-002841-31.
Keywords: biomarkers, tumor; immunotherapy; non-small cell lung cancer.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GLR provided consultation, attended advisory boards and/or provided lectures for the following organizations, from whom received honoraria or education grants: Merck Sharp and Dohme, Takeda, Amgen, Eli Lilly, BMS, Roche, Italfarmaco, Novartis, Sanofi, Pfizer and AstraZeneca. AP declares personal fees from AstraZeneca, Italfarmaco, Roche, BMS. RF declares advisory role from Merck Sharp and Dohme. FDB provided consultation, attended advisory boards and/or provided lectures for the following organizations, from whom received honoraria or education grants: Amgen, AstraZeneca, Boehringer-Ingelheim, BMS, Eli Lilly, F. Hoffmann-La Roche, Ignyta, Merck Sharp and Dohme, Merck Serono, Novartis, Pfizer.CP declares personal fees from Italfarmaco, AstraZeneca, BMS and Merck Sharp and Dohme.MCG declares personal financial interests with the following organizations: AstraZeneca, MSD International GmbH, BMS, Boehringer Ingelheim Italia S.p.A, Celgene, Eli Lilly, Ignyta, Incyte, Inivata, MedImmune, Novartis, Pfizer, Roche, Takeda, Seattle Genetics, Mirati, Daiichi Sankyo, Regeneron, Merck, Ose Immuno Therapeutics, Blueprint, Jansenn, Sanofi; she also declares Institutional financial interests with the following organizations: Eli Lilly, MSD, Pfizer (MISP); AstraZeneca, MSD International GmbH, BMS, Boehringer Ingelheim Italia S.p.A, Celgene, Eli Lilly, Ignyta, Incyte, MedImmune, Novartis, Pfizer, Roche, Takeda, Tiziana, Foundation Medicine, Glaxo Smith Kline GSK, Spectrum pharmaceuticals.
Figures

Comment in
-
Unravelling the puzzle of immunotherapeutic efficacy in lung cancer.Transl Lung Cancer Res. 2024 May 31;13(5):1173-1176. doi: 10.21037/tlcr-24-221. Epub 2024 May 17. Transl Lung Cancer Res. 2024. PMID: 38854949 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous