

Final results of DESTINY-CRC01 investigating trastuzumab deruxtecan in patients with HER2-expressing metastatic colorectal cancer
- PMID: 37286557
- PMCID: PMC10247780
- DOI: 10.1038/s41467-023-38032-4
Final results of DESTINY-CRC01 investigating trastuzumab deruxtecan in patients with HER2-expressing metastatic colorectal cancer
Abstract
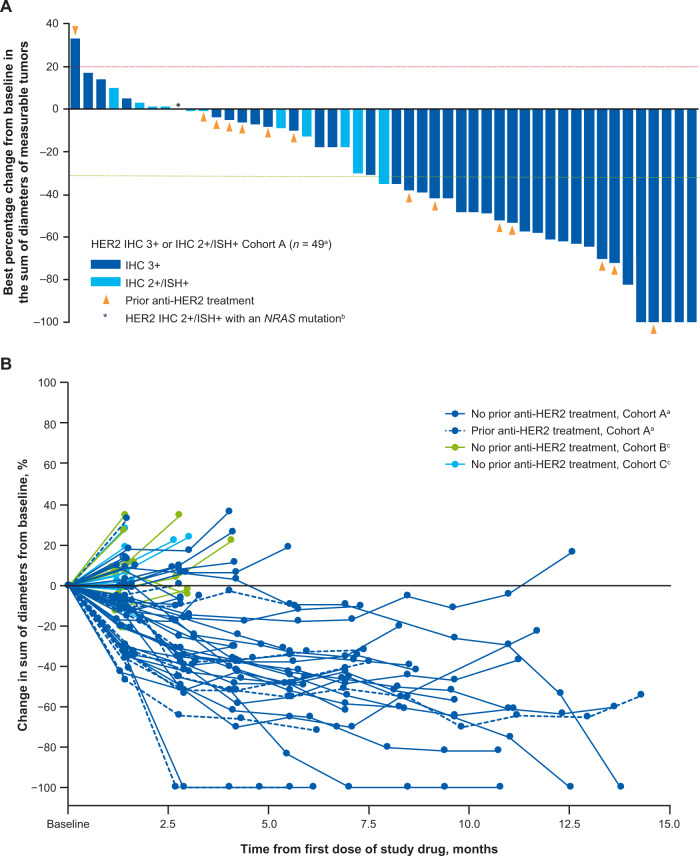
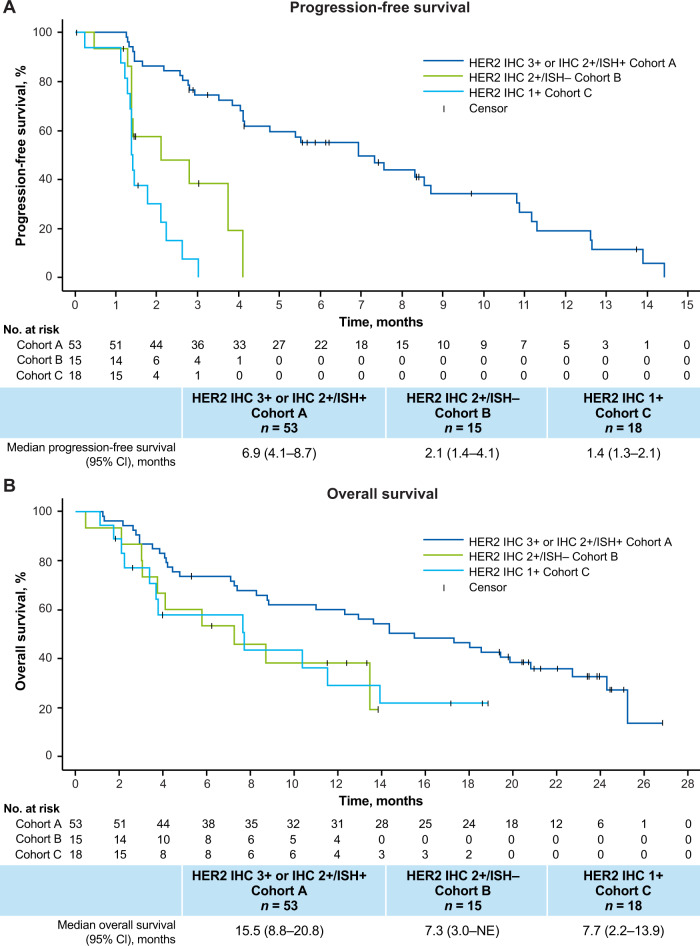
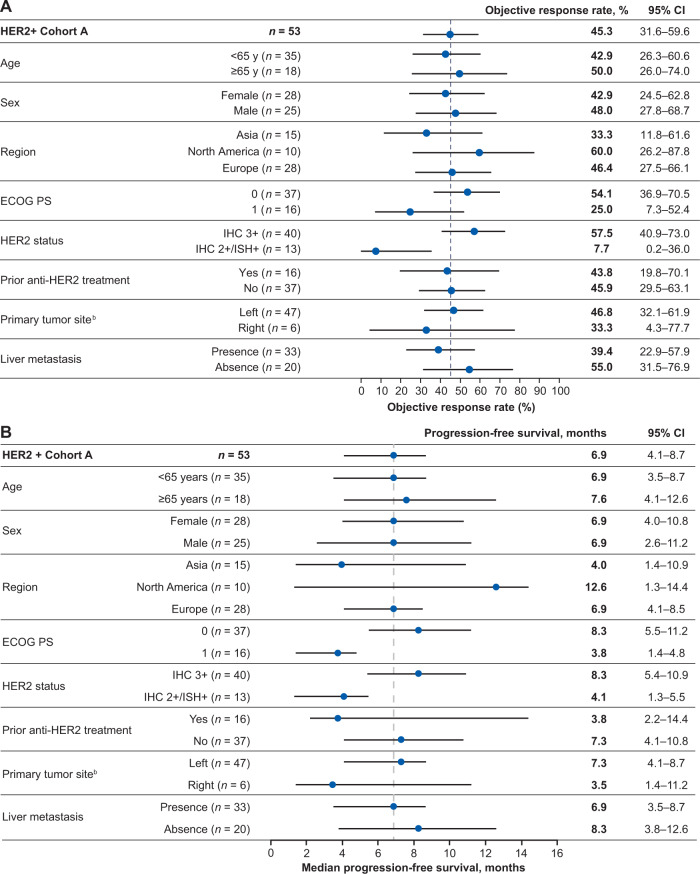
DESTINY-CRC01 (NCT03384940) was a multicenter, open-label, phase 2 trial assessing the efficacy and safety of trastuzumab deruxtecan (T-DXd) in patients with HER2-expressing metastatic colorectal cancer (mCRC) that progressed after ≥2 prior regimens; results of the primary analysis are published. Patients received T-DXd 6.4 mg/kg every 3 weeks and were assigned to either: cohort A (HER2-positive, immunohistochemistry [IHC] 3+ or IHC 2+/in situ hybridization [ISH]+), cohort B (IHC 2+/ISH-), or cohort C (IHC 1+). Primary endpoint was objective response rate (ORR) by independent central review in cohort A. Secondary endpoints included ORR (cohorts B and C), duration of response, disease control rate, progression-free survival, overall survival, pharmacokinetics, and safety of T-DXd. 86 patients were enrolled (53 in cohort A, 15 in cohort B, and 18 in cohort C). Results of the primary analysis are published, reporting an ORR of 45.3% in cohort A. Here, we report the final results. No responses occurred in cohorts B or C. Median progression-free survival, overall survival, and duration of response were 6.9, 15.5, and 7.0 months, respectively. Overall serum exposure (cycle 1) of T-DXd, total anti-HER2 antibody, and DXd were similar regardless of HER2 status. Most common grade ≥3 treatment-emergent adverse events were decreased neutrophil count and anemia. Adjudicated drug-related interstitial lung disease/pneumonitis occurred in 8 patients (9.3%). These findings support the continued exploration of T-DXd in HER2-positive mCRC.
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: T.Y. has received support for the present manuscript from Daiichi Sankyo and has received institutional grants or contracts from Taiho Pharmaceutical, Sumitomo Dainippon, Ono Pharmaceutical, Chugai Pharmaceutical, Amgen, Parexel International MSD, and Sanofi KK. M.D.B. has received research funding, provision of study materials, medical writing, and article processing charges from Daiichi Sankyo. K.R. has received institutional research funding from Daiichi Sankyo; has received grants or contracts from Roche/Genentech; and has received honoraria for lectures, presentations, speaker bureaus, manuscript writing, or educational events from Daiichi Sankyo. T.M. has received institutional grants or contracts from MSD, Daiichi Sankyo, Ono Pharmaceuticals, and Novartis, and has received honoraria from Takeda, Chugai Pharmaceuticals, Merck Bio Pharma, Taiho, Bayer, Eli Lilly Japan KK, Yakult Honsha, Sanofi, Daiichi Sankyo, Ono Pharmaceuticals, and BMS. H.K. has received grants or contracts from Chugai Pharmaceuticals, Taiho Pharmaceuticals, and Eisai Co. Ltd; has received consulting fees from BMS, Eli Lilly Japan KK, Ono Pharmaceuticals, Daiichi Sankyo, and Taiho Pharmaceuticals; and has received honoraria from BMS, Bayer Yakuhin Ltd, Eli Lilly Japan KK, MSD KK, Ono Pharmaceuticals, Chugai Pharmaceuticals, Daiichi Sankyo, Takeda Pharmaceuticals, and Taiho Pharmaceuticals. K.Y. has received institutional support for the present manuscript from Daiichi Sankyo and has received honoraria for lectures from Daiichi Sankyo. T.N. has received institutional support for the present manuscript from Daiichi Sankyo and has received honoraria from Ono Pharmaceuticals, Taiho Pharmaceuticals, Takeda Pharmaceuticals, Chugai Pharmaceuticals, and Daiichi Sankyo. Z.W. has received consulting fees from Merck, Ibsen, Eli Lilly, Five Prime, QED, Molecular Templates, Daiichi Sankyo, AstraZeneca, Bayer, Novartis; has received support for attending meetings and/or travel from Lilly, Merck, Novartis, and Daiichi Sankyo; and has participated on a data safety monitory board or advisory board for Array. E.E. has received grants or contracts from F. Hoffman La-Roche, BMS, Servier, Amgen, Merck Serono, Array Biopharma, Sanofi, and Bayer; institutional funds for grants from Array Biopharma, MSD, AbbVie, Amgen, GlaxoSmithKline, AstraZeneca, Merck Sharpe and Dohme Corp, BMS, Novartis, Boehringer Ingelheim, Hoffman La-Roche, MedImmune, Pierre-Fabre, and Sanofi Aventis; has received consulting fees from Hoffman La-Roche, BMS, Servier, Amgen, Merck Serono, Array Biopharma, Sanofi, Bayer; has received honoraria from F. Hoffman La-Roche, BMS, Servier, Amgen, Merck Serono, Array Biopharma, Sanofi, Bayer; has received payment for expert testimony from F. Hoffman La-Roche, BMS, Servier, Amgen, Merck Serono, Array Biopharma, Sanofi, Bayer; and has received support for attending meetings and/or travel from F. Hoffman La-Roche, BMS, Amgen, Merck Serono, Array Biopharma, Sanofi, Bayer. M.F. has received institutional grants or contracts from AstraZeneca, Novartis, and Amgen; has received consulting fees from HalioDx, Incyte Corporation, Mirati, Pfizer, Taiho, and Zhuhai Yufan Biotech; has received honoraria from Amgen and Guardant360; and has participated on a data safety monitoring board or advisory board for Amgen, Seattle Genetics, GlaxoSmithKline, Array Biopharma, Mirati, and Bayer. F.C. has served as an advisor and speaker for Roche, Amgen, Merck Serono, Pfizer, Sanofi, Bayer, Servier, Bristol Myers Squibb, Celgene, and Eli Lilly; and received institutional research grants from Bayer, Roche, Merck Serono, Amgen, AstraZeneca, and Takeda. A.G. has received institutional medical writing support from Daiichi Sankyo; has received consulting fees from Daiichi Sankyo, Bayer, Merck/MSD, Genentech/Roche, Natera, and BMS; has received honoraria for lectures, presentations, speaker bureaus, manuscript writing or educational events from Bayer, Genentech/Roche, and Merck/MSD; and has participated on a data safety monitoring board or advisory board for Regeneron. K.S., K.K., E.B., Y.O., and G.M. are full-time employees of Daiichi Sankyo. F.L., J.R., and S.S. have nothing to declare.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
