

Elevated plasma complement factor H related 5 protein is associated with venous thromboembolism
- PMID: 37286573
- PMCID: PMC10247781
- DOI: 10.1038/s41467-023-38383-y
Elevated plasma complement factor H related 5 protein is associated with venous thromboembolism
Erratum in
-
Author Correction: Elevated plasma complement factor H related 5 protein is associated with venous thromboembolism.Nat Commun. 2023 Nov 27;14(1):7752. doi: 10.1038/s41467-023-43764-4. Nat Commun. 2023. PMID: 38012230 Free PMC article. No abstract available.
Abstract
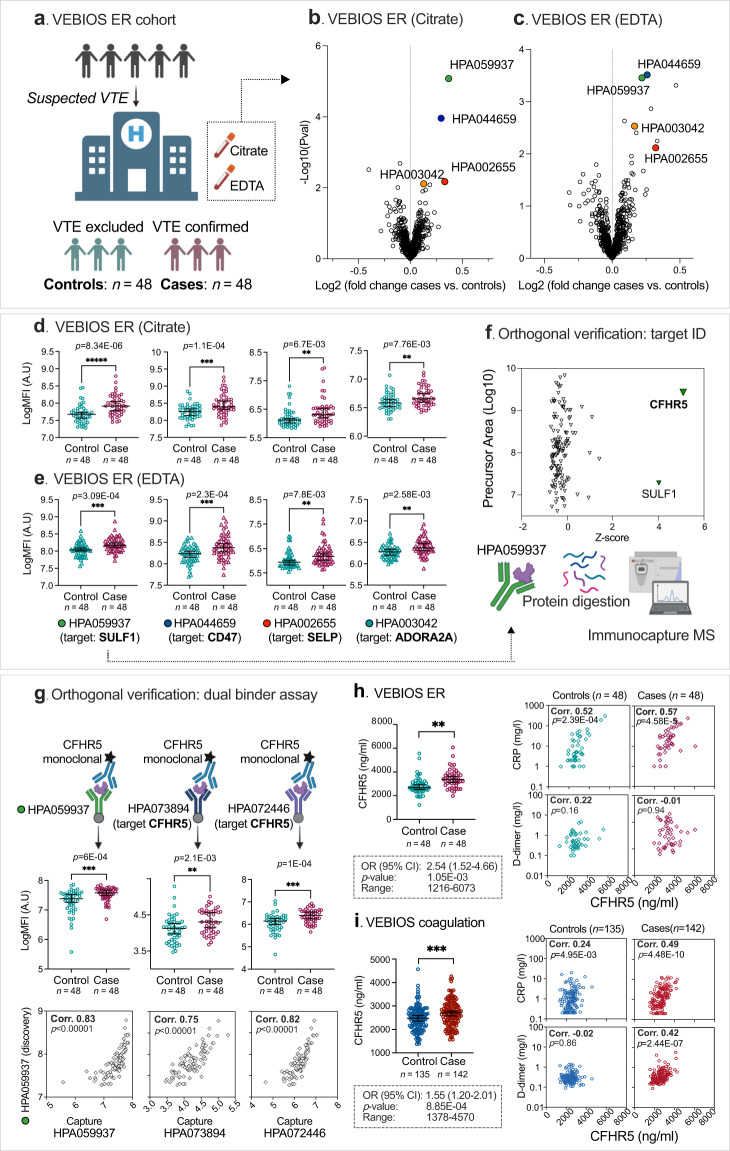
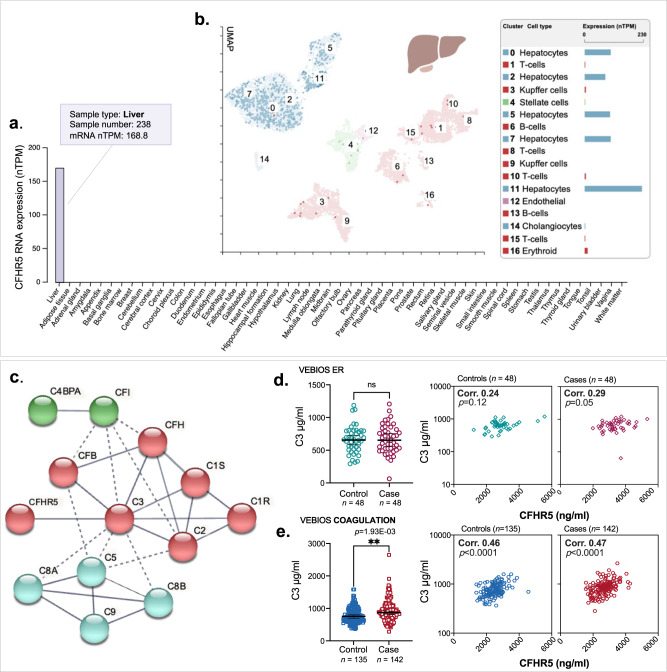
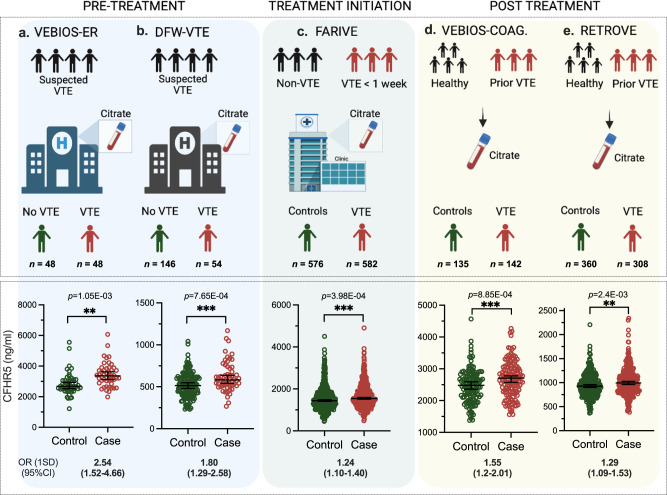
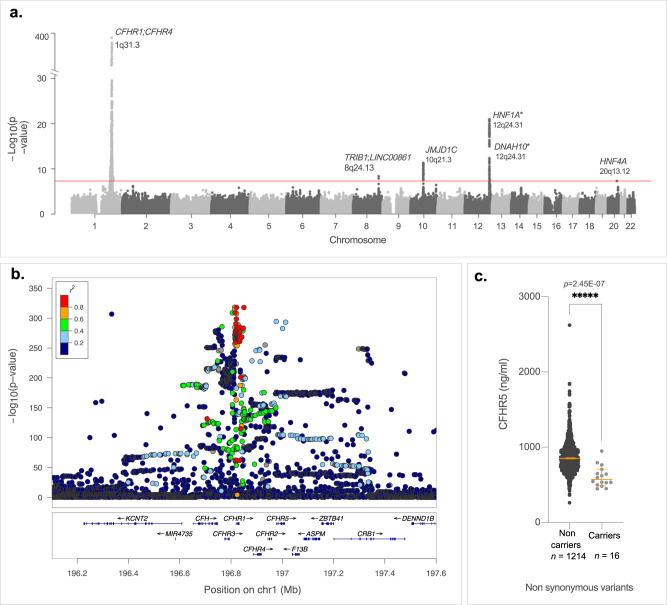
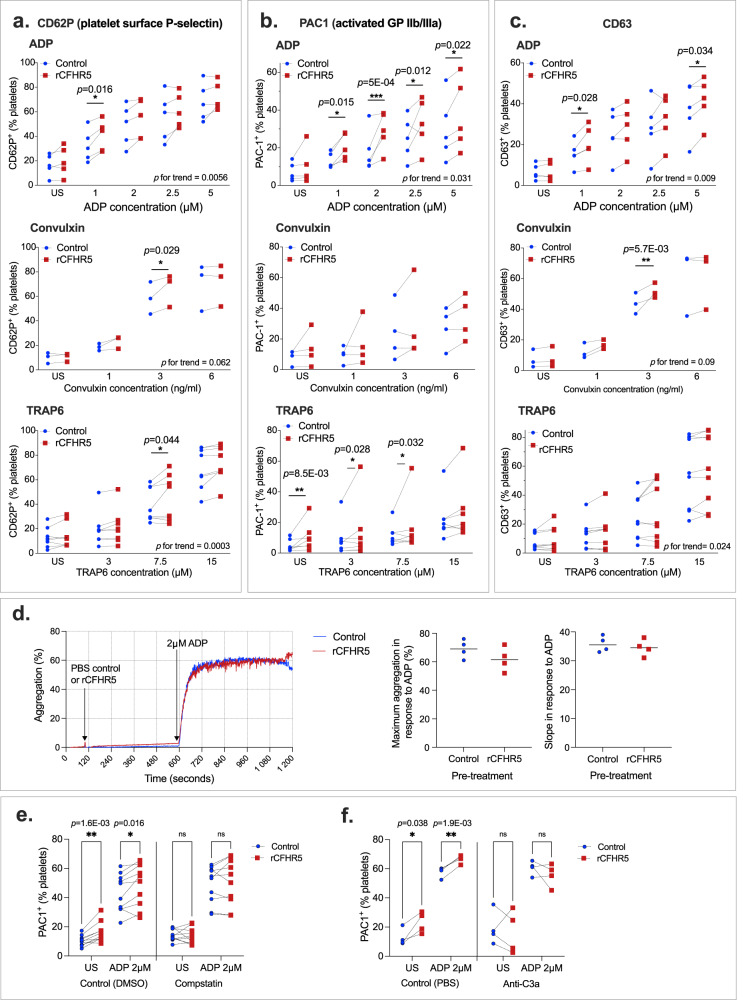
Venous thromboembolism (VTE) is a common, multi-causal disease with potentially serious short- and long-term complications. In clinical practice, there is a need for improved plasma biomarker-based tools for VTE diagnosis and risk prediction. Here we show, using proteomics profiling to screen plasma from patients with suspected acute VTE, and several case-control studies for VTE, how Complement Factor H Related 5 protein (CFHR5), a regulator of the alternative pathway of complement activation, is a VTE-associated plasma biomarker. In plasma, higher CFHR5 levels are associated with increased thrombin generation potential and recombinant CFHR5 enhanced platelet activation in vitro. GWAS analysis of ~52,000 participants identifies six loci associated with CFHR5 plasma levels, but Mendelian randomization do not demonstrate causality between CFHR5 and VTE. Our results indicate an important role for the regulation of the alternative pathway of complement activation in VTE and that CFHR5 represents a potential diagnostic and/or risk predictive plasma biomarker.
© 2023. The Author(s).
Conflict of interest statement
Dr. Klarin is a scientific advisor and reports consulting fees from Bitterroot Bio, Inc unrelated to the present work. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
