

Evaluation of Schlemm's canal with swept-source optical coherence tomography in primary angle-closure disease
- PMID: 37286943
- PMCID: PMC10245448
- DOI: 10.1186/s12886-023-03001-4
Evaluation of Schlemm's canal with swept-source optical coherence tomography in primary angle-closure disease
Erratum in
-
Correction: Evaluation of Schlemm's canal with swept-source optical coherence tomography in primary angle-closure disease.BMC Ophthalmol. 2023 Jul 10;23(1):308. doi: 10.1186/s12886-023-03062-5. BMC Ophthalmol. 2023. PMID: 37430214 Free PMC article. No abstract available.
Abstract
Purpose: To perform an in vivo evaluation of the changes in Schlemm's canal (SC) among patients with primary angle-closure disease (PACD) using swept-source optical coherence tomography (SS-OCT).
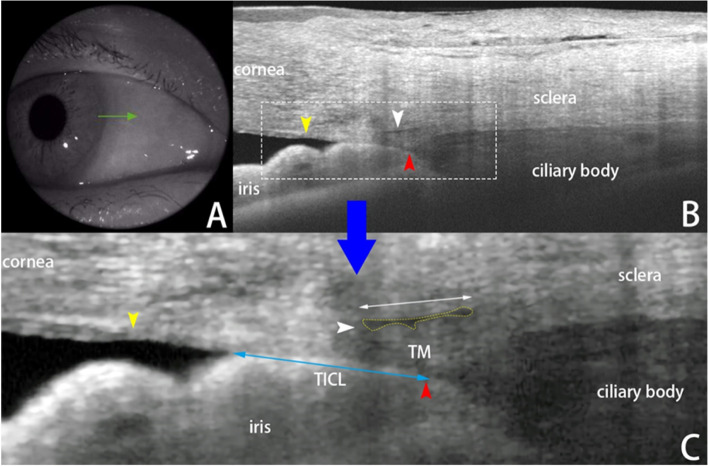
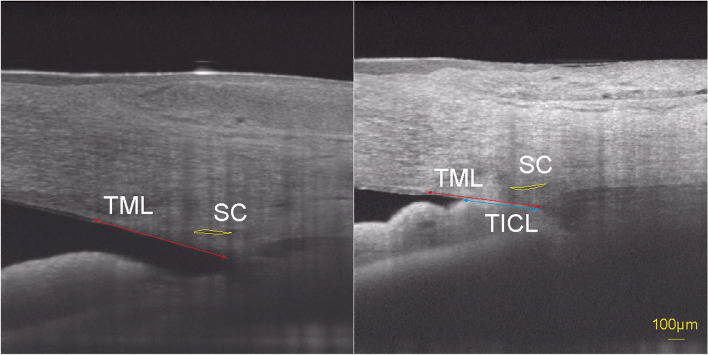
Methods: Patients diagnosed with PACD who had not undergone surgery were recruited. The SS-OCT quadrants scanned herein included the nasal and temporal sections at 3 and 9 o'clock, respectively. The diameter and cross-sectional area of the SC were measured. A linear mixed-effects model was performed to analyze the effects of parameters on the SC changes. The hypothesis of interest was related to the angle status (iridotrabecular contact, ITC/open angle, OPN), which was further explored with pairwise comparisons of the estimated marginal means (EMMs) of the SC diameter and SC area. In the ITC regions, the relationship between the trabecular-iris contact length (TICL) percentage and SC parameters was also studied by a mixed model.
Results: A total of 49 eyes of 35 patients were included for measurements and analysis. The percentage of observable SCs in the ITC regions was only 58.5% (24/41), whereas it was 86.0% (49/57) in the OPN regions (χ2 = 9.44, p = 0.002). ITC was significantly associated with a decreasing SC size. The EMMs for the diameter and cross-sectional area of SC at the ITC and OPN regions were 203.34 μm versus 261.41 μm (p = 0.006) and 3174.43 μm2 versus 5347.63 μm2 (p = 0.022), respectively. Sex, age, spherical equivalent refraction, intraocular pressure, axial length, extent of angle closure, history of acute attack and treatment with LPI were not significantly associated with SC parameters. In the ITC regions, a larger TICL percentage was significantly associated with a decrease in SC diameter and area (p = 0.003 and 0.019, respectively).
Conclusions: The morphologies of SC could be affected by the angle status (ITC/OPN) in patients with PACD, and ITC was significantly associated with a decreasing SC size. These changes in SC as described by OCT scans might help to elucidate the progression mechanisms of PACD.
Keywords: Iridotrabecular contact; Optical coherence tomography; Primary angle closure disease; Schlemm’s canal.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Grant WM. Clinical measurements of aqueous outflow. Am J Ophthalmol. 1951;34(11):1603–1605. - PubMed
MeSH terms
Grants and funding
- 81970796,82171046,82101114/National Natural Science Foundation of China
- 81970796,82171046,82101114/National Natural Science Foundation of China
- YG2019QNA18/Cross disciplinary Research Fund of Shanghai Ninth People's Hospital, Shanghai JiaoTong university School of Medicine
- 201940330/Clinical Research Program of Shanghai Municipal Health Commission
- JYLJ201905/Clinical Research Program of 9th People's Hospital affiliated to Shanghai Jiao Tong University School of Medicine
LinkOut - more resources
Full Text Sources
Research Materials
