

Chromosomal radiosensitivity in oncological and non-oncological patients with rheumatoid arthritis and connective tissue diseases
- PMID: 37287050
- PMCID: PMC10249309
- DOI: 10.1186/s13014-023-02291-8
Chromosomal radiosensitivity in oncological and non-oncological patients with rheumatoid arthritis and connective tissue diseases
Abstract
Background: The risk of developing late radiotoxicity after radiotherapy in patients with high chromosomal radiosensitivity after radiotherapy could potentially be higher compared to the risk in patients with average radiosensitivity. In case of extremely high radiosensitivity, dose reduction may be appropriate. Some rheumatic diseases (RhD), including connective tissue diseases (CTDs) appear to be associated with higher radiosensitivity. The question arises as to whether patients with rheumatoid arthritis (RA) also generally have a higher radiosensitivity and whether certain parameters could indicate clues to high radiosensitivity in RA patients which would then need to be further assessed before radiotherapy.
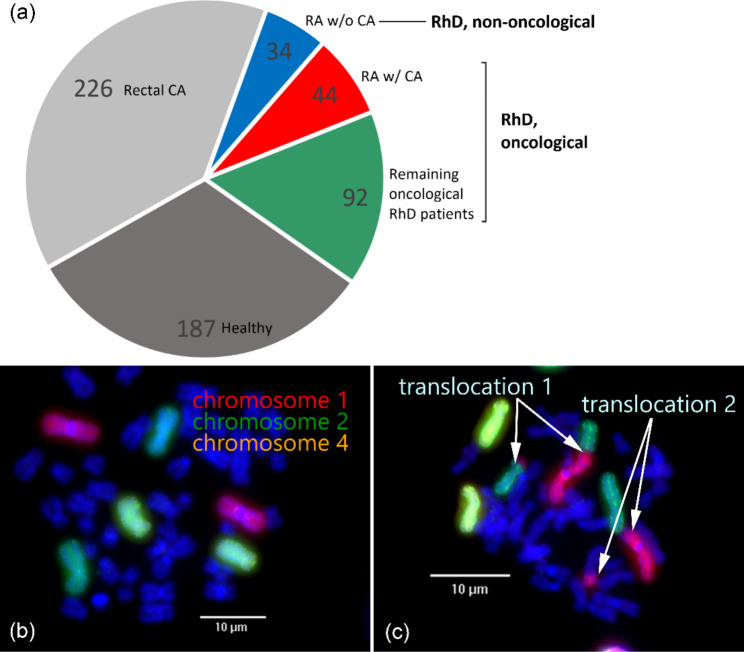
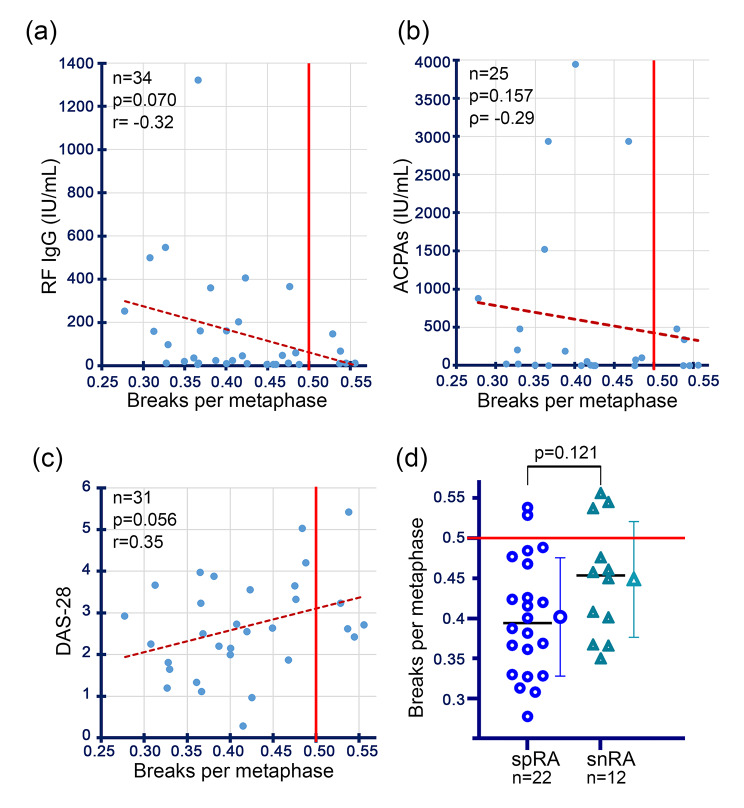
Methods: Radiosensitivity was determined in 136 oncological patients with RhD, 44 of whom were RA patients, and additionally in 34 non-oncological RA patients by three-colour fluorescence in situ hybridization (FiSH), in which lymphocyte chromosomes isolated from peripheral blood are analysed for their chromosomal aberrations of an unirradiated and an with 2 Gy irradiated blood sample. The chromosomal radiosensitivity was determined by the average number of breaks per metaphase. In addition, correlations between certain RA- or RhD-relevant disease parameters or clinical features such as the disease activity score 28 and radiosensitivity were assessed.
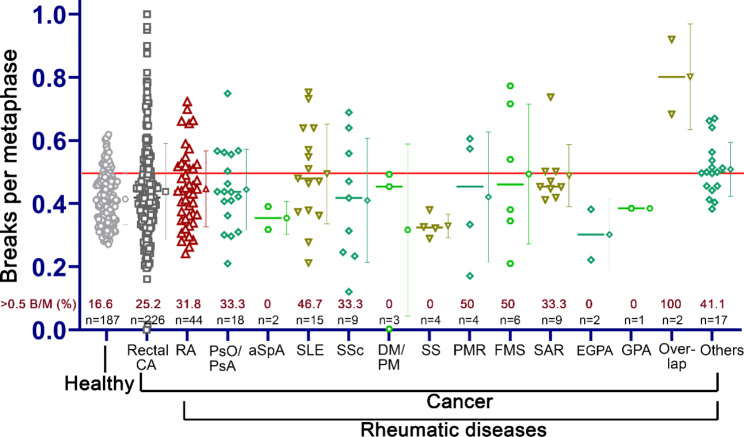
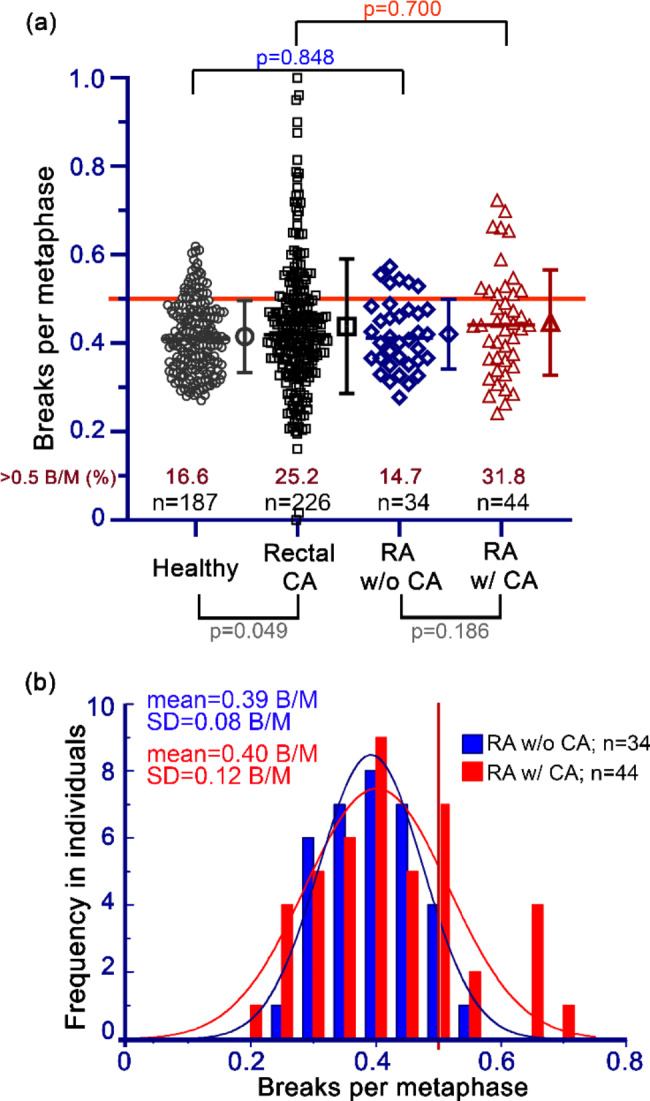
Results: Some oncological patients with RhD, especially those with connective tissue diseases have significantly higher radiosensitivity compared with oncology patients without RhD. In contrast, the mean radiosensitivity of the oncological patients with RA and other RhD and the non-oncological RA did not differ. 14 of the 44 examined oncological RA-patients (31.8%) had a high radiosensitivity which is defined as ≥ 0.5 breaks per metaphase. No correlation of laboratory parameters with radiosensitivity could be established.
Conclusions: It would be recommended to perform radiosensitivity testing in patients with connective tissue diseases in general. We did not find a higher radiosensitivity in RA patients. In the group of RA patients with an oncological disease, a higher percentage of patients showed higher radiosensitivity, although the average radiosensitivity was not high.
Keywords: Chromosomal aberrations; Collagen vascular disease; Connective tissue disease; Fluorescence in situ hybridisation; Radiation sensitivity; Radiosensitivity; Radiotherapy; Radiotoxicity; Rheumatism; Rheumatoid arthritis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Distel LV, Neubauer S, Keller U, Sprung CN, Sauer R, Grabenbauer GG. Individual differences in chromosomal aberrations after in vitro irradiation of cells from healthy individuals, cancer and cancer susceptibility syndrome patients. Radiother Oncol. 2006;81:257–63. doi: 10.1016/j.radonc.2006.10.012. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
