

Automatic localisation and per-region quantification of traumatic brain injury on head CT using atlas mapping
- PMID: 37287542
- PMCID: PMC10241839
- DOI: 10.1016/j.ejro.2023.100491
Automatic localisation and per-region quantification of traumatic brain injury on head CT using atlas mapping
Abstract
Rationale and objectives: To develop a method for automatic localisation of brain lesions on head CT, suitable for both population-level analysis and lesion management in a clinical setting.
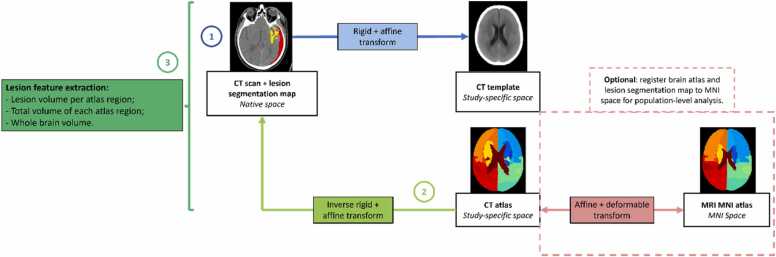
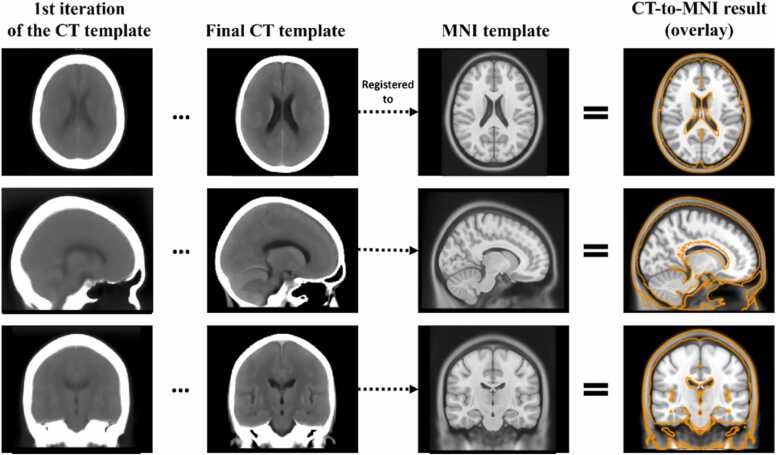
Materials and methods: Lesions were located by mapping a bespoke CT brain atlas to the patient's head CT in which lesions had been previously segmented. The atlas mapping was achieved through robust intensity-based registration enabling the calculation of per-region lesion volumes. Quality control (QC) metrics were derived for automatic detection of failure cases. The CT brain template was built using 182 non-lesioned CT scans and an iterative template construction strategy. Individual brain regions in the CT template were defined via non-linear registration of an existing MRI-based brain atlas.Evaluation was performed on a multi-centre traumatic brain injury dataset (TBI) (n = 839 scans), including visual inspection by a trained expert. Two population-level analyses are presented as proof-of-concept: a spatial assessment of lesion prevalence, and an exploration of the distribution of lesion volume per brain region, stratified by clinical outcome.
Results: 95.7% of the lesion localisation results were rated by a trained expert as suitable for approximate anatomical correspondence between lesions and brain regions, and 72.5% for more quantitatively accurate estimates of regional lesion load. The classification performance of the automatic QC showed an AUC of 0.84 when compared to binarised visual inspection scores. The localisation method has been integrated into the publicly available Brain Lesion Analysis and Segmentation Tool for CT (BLAST-CT).
Conclusion: Automatic lesion localisation with reliable QC metrics is feasible and can be used for patient-level quantitative analysis of TBI, as well as for large-scale population analysis due to its computational efficiency (<2 min/scan on GPU).
Keywords: CT; Image registration; Traumatic brain injury.
© 2023 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Prof. Ben Glocker reports financial support was provided by European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation program (Grant Agreement No. 757173, Project MIRA). The CENTER-TBI study was supported by the European Union 7th Framework Programme (EC grant 602150). Carolina Piçarra and Stefan Winzeck report financial support provided by UKRI London Medical Imaging & Artificial Intelligence Centre for Value Based Healthcare. Virginia Newcombe reports financial support was provided by Academy of Medical Sciences.
Figures




References
-
- Dewan Michael C., et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018;130(4):1080–1097. - PubMed
-
- Rowe Brian H., et al. Concussion diagnoses among adults presenting to three Canadian emergency departments: missed opportunities. Am. J. Emerg. Med. 2018;36(12):2144–2151. - PubMed
Further reading
-
- Christian Ledig, et al. Robust whole-brain segmentation: application t traumatic brain injury. Med. Image Anal. 2015;21(1):40–58. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
