

A rare radiological presentation of pulmonary metastases from malignant melanoma
- PMID: 37287725
- PMCID: PMC10241655
- DOI: 10.1016/j.radcr.2023.04.060
A rare radiological presentation of pulmonary metastases from malignant melanoma
Abstract
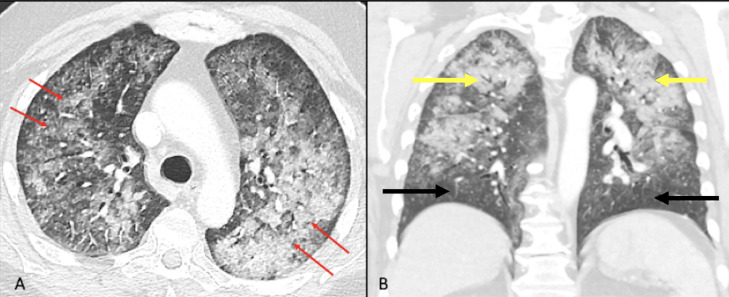
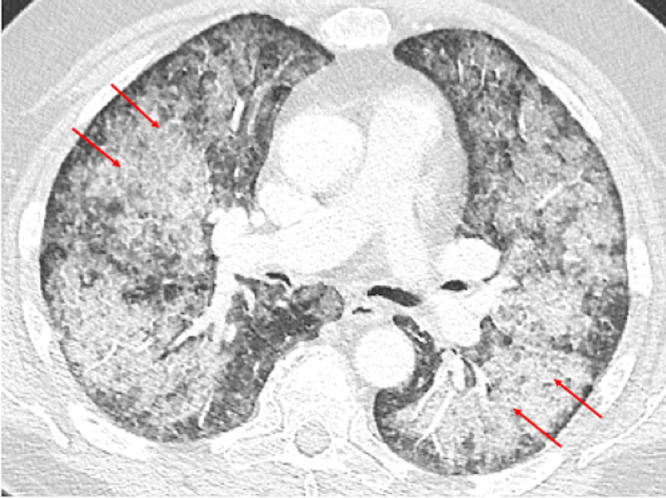
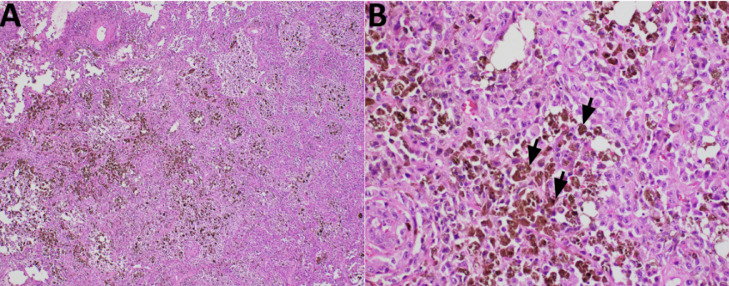
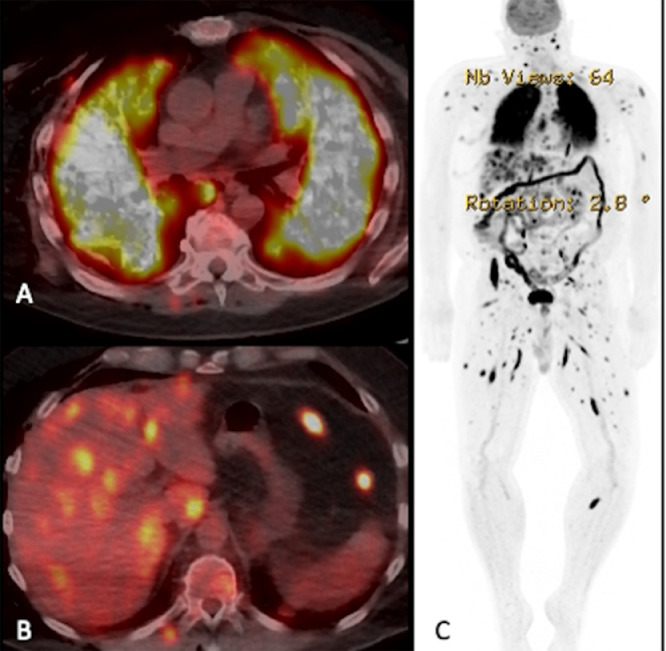
Malignant melanoma is a highly aggressive cancer with metastatic potential to various locations such as the lymph nodes, lungs, liver, brain, and bone. After the lymph nodes, the lungs are the most common site of malignant melanoma metastases. Pulmonary metastases from malignant melanoma commonly presents as solitary or multiple solid nodules, sub-solid nodules or miliary opacities on CT chest. We present a case of pulmonary metastases from malignant melanoma in a 74-year-old man which presented unusually on CT chest as a combination of patterns like "crazy paving," upper lobe predominance with subpleural sparing, and centrilobular micronodules. Video-assisted thoracoscopic surgery, wedge resection and tissue analysis were performed, which confirmed the diagnosis of malignant melanoma metastases, and the patient further underwent PET-CT for staging and surveillance. Patients with pulmonary metastases from malignant melanoma can have atypical imaging findings, therefore radiologists should be aware of these unconventional presentations to avoid any misdiagnoses.
Keywords: Atypical presentation; Crazy paving; Malignant melanoma; Oncology; Pulmonary metastases.
© 2023 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
