

NET-02: a randomised, non-comparative, phase II trial of nal-IRI/5-FU or docetaxel as second-line therapy in patients with progressive poorly differentiated extra-pulmonary neuroendocrine carcinoma
- PMID: 37287870
- PMCID: PMC10242623
- DOI: 10.1016/j.eclinm.2023.102015
NET-02: a randomised, non-comparative, phase II trial of nal-IRI/5-FU or docetaxel as second-line therapy in patients with progressive poorly differentiated extra-pulmonary neuroendocrine carcinoma
Abstract
Background: The prognosis for patients with poorly-differentiated extra-pulmonary neuroendocrine carcinoma (PD-EP-NEC) is poor. A recognised first-line (1L) treatment for advanced disease is etoposide/platinum-based chemotherapy with no standard second-line (2L) treatment.
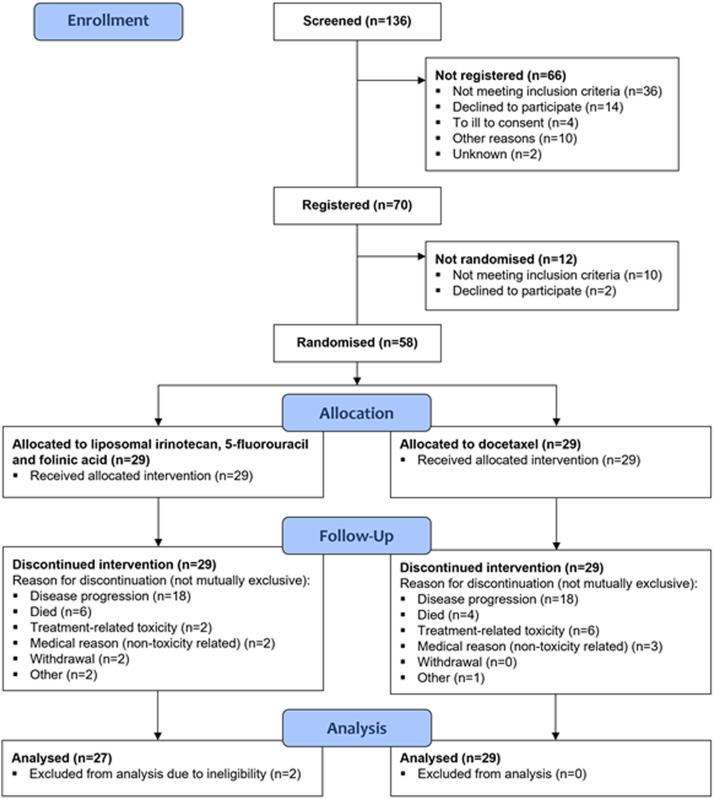
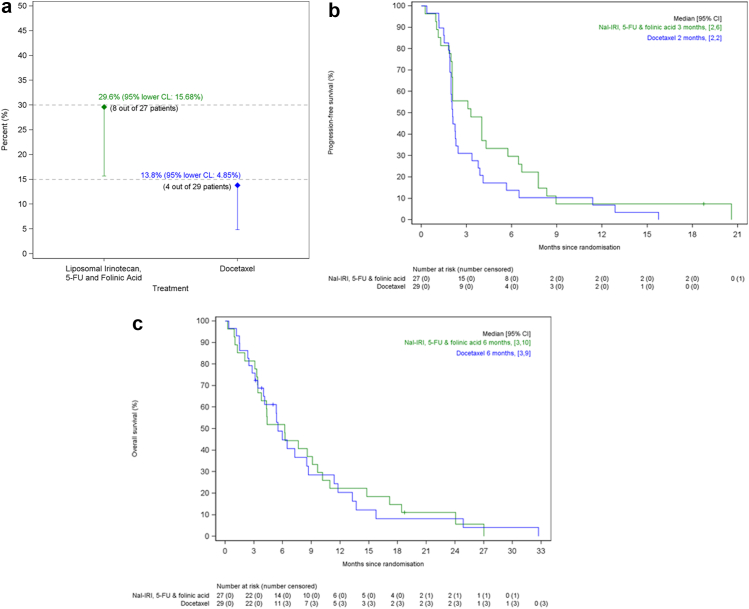
Methods: Patients with histologically-confirmed PD-EP-NEC (Ki-67 > 20%; Grade 3) received IV liposomal irinotecan (nal-IRI) (70 mg/m2 free base)/5-FU (2400 mg/m2)/folinic acid, Q14 days (ARM A), or IV docetaxel (75 mg/m2), Q21 days (ARM B), as 2L therapy. Primary endpoint was 6-month progression-free survival (PFS) rate (80% power to demonstrate one-sided 95% lower confidence interval excluded 15% (target level of efficacy: 30%)). Secondary endpoints: objective response rate (ORR), median PFS, overall survival (OS), toxicity and patient-reported quality-of-life (QoL) (ClinicalTrials.gov: NCT03837977).
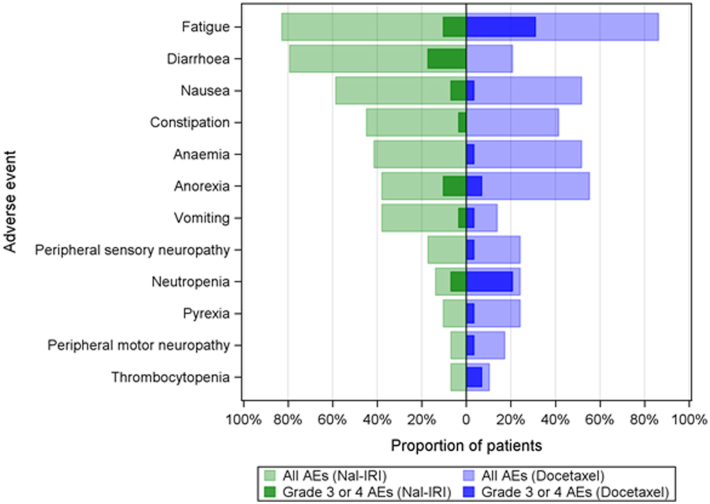
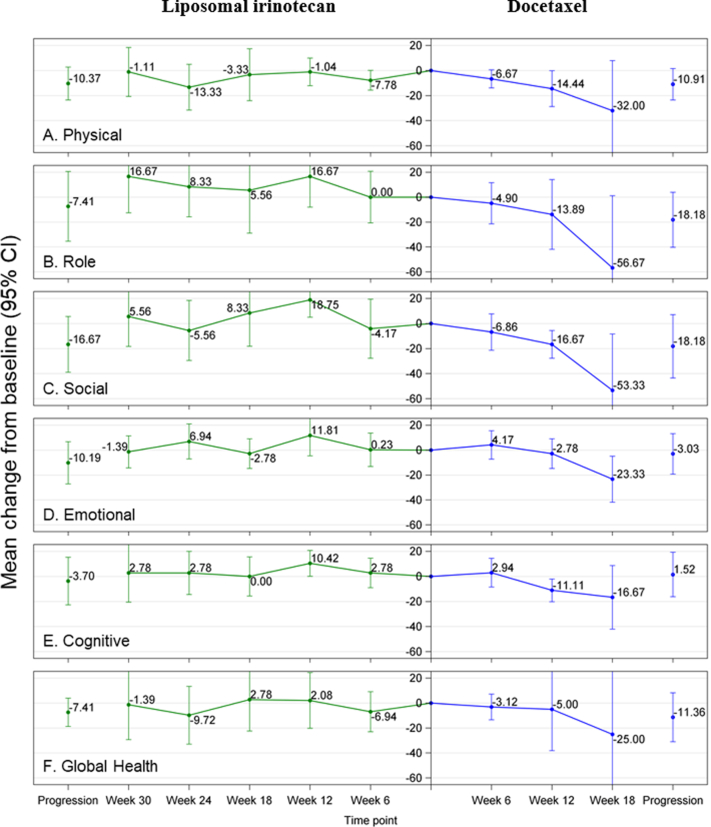
Findings: Of 58 patients (29 each arm); 57% male, 90% ECOG PS 0/1, 10% PS 2, 89.7% Ki-67 ≥ 55%, primary site: 70.7%-gastrointestinal, 18.9%-other, 10.3%-unknown, 91.4%/6.9%/1.7% were resistant/sensitive/intolerant to 1L platinum-based treatment, respectively. The primary end-point of 6-month PFS rate was met by ARM A: 29.6% (lower 95% Confidence-Limit (CL) 15.7), but not by ARM B: 13.8% (lower 95%CL:4.9). ORR, median PFS and OS were 11.1% (95%CI:2.4-29.2) and 10.3% (95%CI:2.2-27.4%); 3 months (95%CI:2-6) and 2 months (95%CI:2-2); and 6 months (95%CI:3-10) and 6 months (95%CI:3-9) in ARMS A and B, respectively. Adverse events ≥ grade 3 occurred in 51.7% and 55.2% (1 and 6 discontinuations due to toxicity in ARMS A and B), respectively. QoL was maintained in ARM A, but not ARM B.
Interpretation: nal-IRI/5-FU/folinic acid, but not docetaxel, met the primary endpoint, with manageable toxicity and maintained QoL, with no difference in OS. ORR and median PFS were similar in both arms. This study provides prospective efficacy, toxicity and QoL data in the 2L setting in a disease group of unmet need, and represents some of the strongest evidence available to recommend systemic treatment to these patients.
Funding: Servier.
Keywords: Docetaxel; Liposomal irinotecan; Neuroendocrine carcinoma; Quality of life; Second-line treatment.
© 2023 The Author(s).
Conflict of interest statement
Mairéad G McNamara: has received research grant support from Servier, Ipsen, NuCana and Astra Zeneca. She has received travel and accommodation support from Advanced Accelerator Applications (UK and Ireland) Ltd, and Ipsen, and speaker honoraria from Advanced Accelerator Applications (UK and Ireland) Ltd.. She has served on advisory boards for Incyte and Astra Zeneca. Jayne Swain: reports grants and non-financial support from Servier, during the conduct of the study. Zoe Craig: reports grants and non-financial support from Servier, during the conduct of the study. Rohini Sharma: has received grant support from AAA, Incyte, Boston Scientific, Bayer and Terumo. She has received speaker honoraria from Roche and Esai. Olusola Faluyi: no conflicts of interest to declare. Jonathan Wadsley: reports grants and personal fees from AstraZeneca, grants and personal fees from Sanofi-Genzyme, speaker and advisory board honoraria from Astrazeneca, Celgene, Novartis, Ipsen, Roche, Bayer, Esteve, Lilly and Eisai. Carys Morgan: no conflicts of interest to declare. Lucy R Wall: no conflicts of interest to declare. Ian Chau: reports advisory role for Eli-Lilly, Bristol Meyers Squibb, MSD, Bayer, Roche, Merck-Serono, Five Prime Therapeutics, AstraZeneca, Oncologie International, Pierre Fabre; research funding from Eli-Lilly, Janssen-Cilag, Sanofi Oncology, Merck-Serono; honorarium from Eli-Lilly. Nick Reed: no conflicts of interest to declare. Debashis Sarker: reports personal fees from MSD, personal fees and non-financial support from EISAI, personal fees and non-financial support from Ipsen, personal fees from Bayer, non-financial support from Mina Therapeutics, personal fees from Pfizer, personal fees from Novartis. Jane Margetts: no conflicts of interest to declare. Daniel Krell: no conflicts of interest to declare. Judith Cave: reports educational support from Amgen. Sharmila Sothi: no conflicts of interest to declare. Alan Anthoney: no conflicts of interest to declare. Chris Bell: no conflicts of interest to declare. Alkesh Patel: no conflicts of interest to declare. Jamie B Oughton: reports grants and/or non-financial support from Servier, Roche, AstraZeneca, Pfizer and Bayer. David Cairns: reports grants and non-financial support from Servier, during the conduct of the study. Wasat Mansoor: no conflicts of interest to declare. Angela Lamarca: has received travel and educational support from Ipsen, Pfizer, Bayer, AAA, SirtEx, Novartis, Mylan and Delcath; speaker honoraria from Merck, Pfizer, Ipsen, Incyte, AAA, QED and Servier; advisory honoraria from EISAI, Nutricia Ipsen, QED, Roche and Servier; she is a member of the Knowledge Network and NET Connect Initiatives funded by Ipsen. Richard A Hubner: has served on the advisory boards for Roche, BMS, Eisai, Celgene, Beigene, Ipsen and BTG. He has received speaker fees from Eisai, Ipsen, Mylan, PrimeOncology and has received travel and educational support from Bayer, BMS and Roche. Juan W Valle: has had consulting or advisory roles for Agios, AstraZeneca, Delcath Systems, Keocyt, Genoscience Pharma, Incyte, Ipsen, Merck, Mundipharma EDO, Novartis, PCI Biotech, Pfizer, Pieris Pharmaceuticals, QED and Wren Laboratories. He is on speakers’ bureaus for Imaging Equipment Limited, Ipsen, Novartis and Nucana; and has received travel grants from Celgene and Nucana.
Figures
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
