

Advanced imaging of fetal cardiac function
- PMID: 37288263
- PMCID: PMC10242056
- DOI: 10.3389/fcvm.2023.1206138
Advanced imaging of fetal cardiac function
Abstract
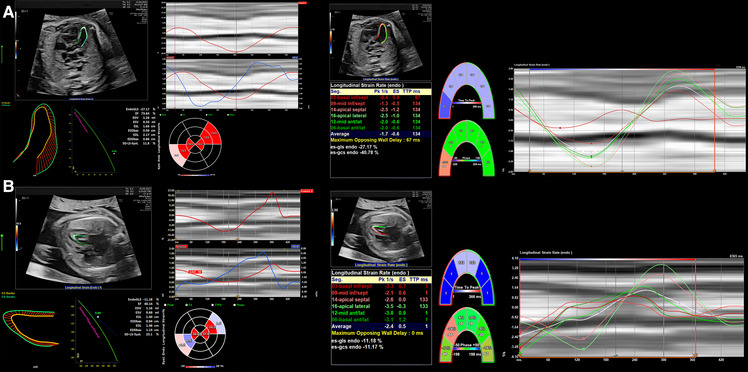
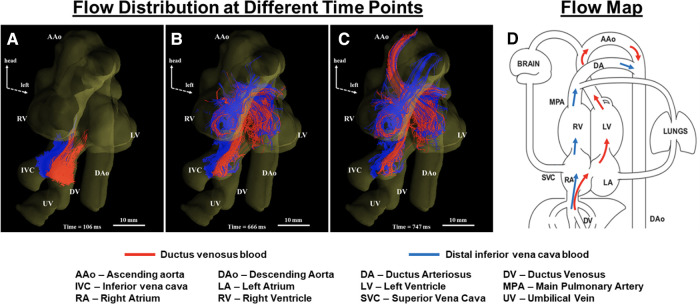
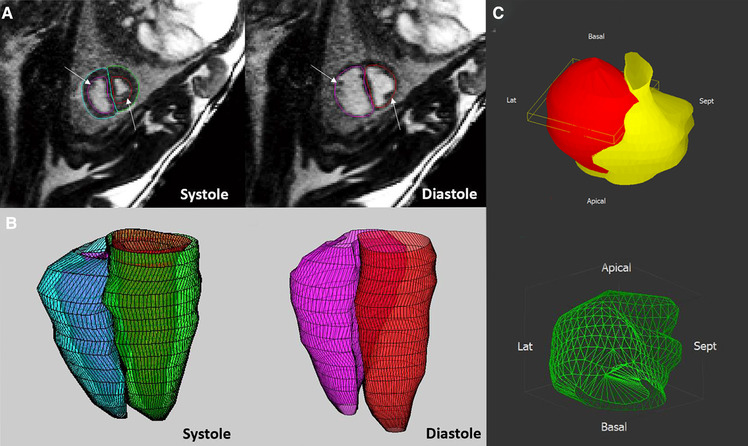
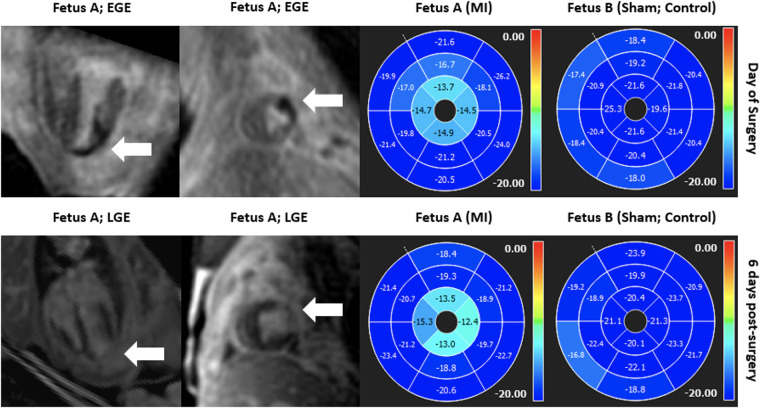
Over recent decades, a variety of advanced imaging techniques for assessing cardiovascular physiology and cardiac function in adults and children have been applied in the fetus. In many cases, technical development has been required to allow feasibility in the fetus, while an appreciation of the unique physiology of the fetal circulation is required for proper interpretation of the findings. This review will focus on recent advances in fetal echocardiography and cardiovascular magnetic resonance (CMR), providing examples of their application in research and clinical settings. We will also consider future directions for these technologies, including their ongoing technical development and potential clinical value.
Keywords: echocardiography; fetal cardiac function; magnetic resonance imaging; speckle tracking; strain.
© 2023 Kühle, Cho, Barber, Goolaub, Darby, Morrison, Haller, Sun and Seed.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Abuhamad A, Chaoui R. A practical guide to fetal echocardiography: Normal and abnormal hearts. 4 edn. Philadelphia: Lippincott Williams & Wilkins; (2022).
Publication types
LinkOut - more resources
Full Text Sources