

The Feasibility, Proficiency, and Mastery Learning Curves in 635 Robotic Pancreatoduodenectomies Following a Multicenter Training Program: "Standing on the Shoulders of Giants"
- PMID: 37288547
- PMCID: PMC10631507
- DOI: 10.1097/SLA.0000000000005928
The Feasibility, Proficiency, and Mastery Learning Curves in 635 Robotic Pancreatoduodenectomies Following a Multicenter Training Program: "Standing on the Shoulders of Giants"
Abstract
Objective: To assess the feasibility, proficiency, and mastery learning curves for robotic pancreatoduodenectomy (RPD) in "second-generation" RPD centers following a multicenter training program adhering to the IDEAL framework.
Background: The long learning curves for RPD reported from "pioneering" expert centers may discourage centers interested in starting an RPD program. However, the feasibility, proficiency, and mastery learning curves may be shorter in "second-generation" centers that participated in dedicated RPD training programs, although data are lacking. We report on the learning curves for RPD in "second-generation" centers trained in a dedicated nationwide program.
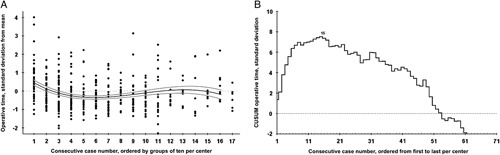
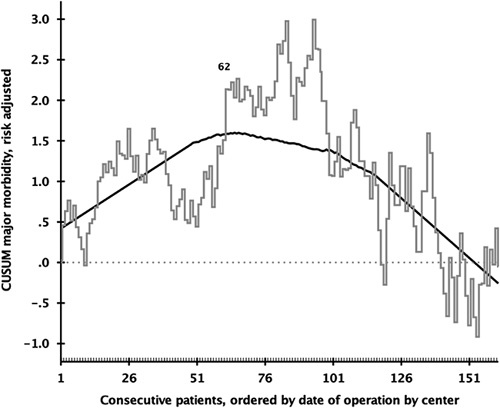
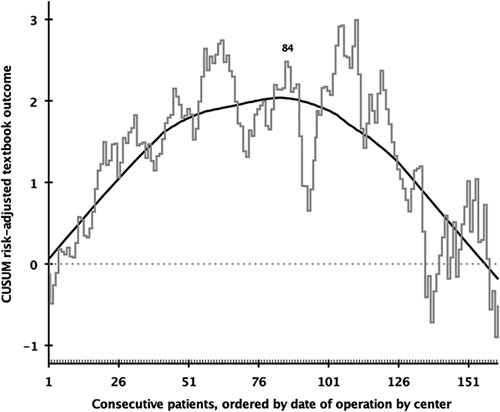
Methods: Post hoc analysis of all consecutive patients undergoing RPD in 7 centers that participated in the LAELAPS-3 training program, each with a minimum annual volume of 50 pancreatoduodenectomies, using the mandatory Dutch Pancreatic Cancer Audit (March 2016-December 2021). Cumulative sum analysis determined cutoffs for the 3 learning curves: operative time for the feasibility (1) risk-adjusted major complication (Clavien-Dindo grade ≥III) for the proficiency, (2) and textbook outcome for the mastery, (3) learning curve. Outcomes before and after the cutoffs were compared for the proficiency and mastery learning curves. A survey was used to assess changes in practice and the most valued "lessons learned."
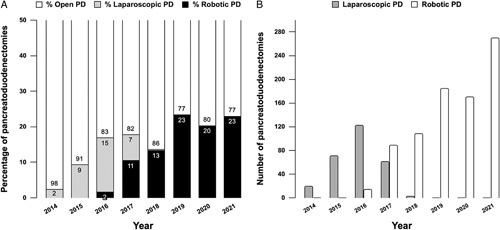
Results: Overall, 635 RPD were performed by 17 trained surgeons, with a conversion rate of 6.6% (n=42). The median annual volume of RPD per center was 22.5±6.8. From 2016 to 2021, the nationwide annual use of RPD increased from 0% to 23% whereas the use of laparoscopic pancreatoduodenectomy decreased from 15% to 0%. The rate of major complications was 36.9% (n=234), surgical site infection 6.3% (n=40), postoperative pancreatic fistula (grade B/C) 26.9% (n=171), and 30-day/in-hospital mortality 3.5% (n=22). Cutoffs for the feasibility, proficiency, and mastery learning curves were reached at 15, 62, and 84 RPD. Major morbidity and 30-day/in-hospital mortality did not differ significantly before and after the cutoffs for the proficiency and mastery learning curves. Previous experience in laparoscopic pancreatoduodenectomy shortened the feasibility (-12 RPDs, -44%), proficiency (-32 RPDs, -34%), and mastery phase learning curve (-34 RPDs, -23%), but did not improve clinical outcome.
Conclusions: The feasibility, proficiency, and mastery learning curves for RPD at 15, 62, and 84 procedures in "second-generation" centers after a multicenter training program were considerably shorter than previously reported from "pioneering" expert centers. The learning curve cutoffs and prior laparoscopic experience did not impact major morbidity and mortality. These findings demonstrate the safety and value of a nationwide training program for RPD in centers with sufficient volume.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
M.J.W.Z. and M.G.B. received funding from Amsterdam UMC for studies on safe implementation of robotic pancreatic surgery; funding from the Dutch Digestive Foundation (Maag Lever Darm Stichting) investigator-initiated studies on minimally invasive pancreatic surgery (Agreement ID: I 16-05); from Intuitive Surgical for the investigator-initiated LAELAPS-3 training program for RPD in the Netherlands for which training suturing material was provided by ETHICON, Johnson & Johnson; from Intuitive for the investigator-initiated LEARNBOT training program for RPD in Europe; funding from Intuitive for the investigator-initiated LIVEROBOT training program for robotic liver surgery in Europe. N.d.G. and M.G.B. received funding from Intuitive® for the DIPLOMA-2 randomized trial on minimally invasive versus open pancreatoduodenectomy. The remaining authors report no conflicts of interest.
Figures
References
-
- Chen S, Chen J-Z, Zhan Q, et al. Robot-assisted laparoscopic versus open pancreaticoduodenectomy: a prospective, matched, mid-term follow-up study. Surg Endosc. 2015;29:3698–3711. - PubMed
-
- Napoli N, Kauffmann EF, Palmeri M, et al. The learning curve in robotic pancreaticoduodenectomy. Dig Surg. 2016;33:299–307. - PubMed
-
- Napoli N, Kauffmann EF, Menonna F, et al. Robotic versus open pancreatoduodenectomy: a propensity score-matched analysis based on factors predictive of postoperative pancreatic fistula. Surg Endosc. 2018;32:1234–1247. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
