

PCI or CABG for left main coronary artery disease: the SWEDEHEART registry
- PMID: 37288564
- PMCID: PMC10406339
- DOI: 10.1093/eurheartj/ehad369
PCI or CABG for left main coronary artery disease: the SWEDEHEART registry
Abstract
Aims: An observational nationwide all-comers prospective register study to analyse outcomes after coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) in unprotected left main coronary artery (LMCA) disease.
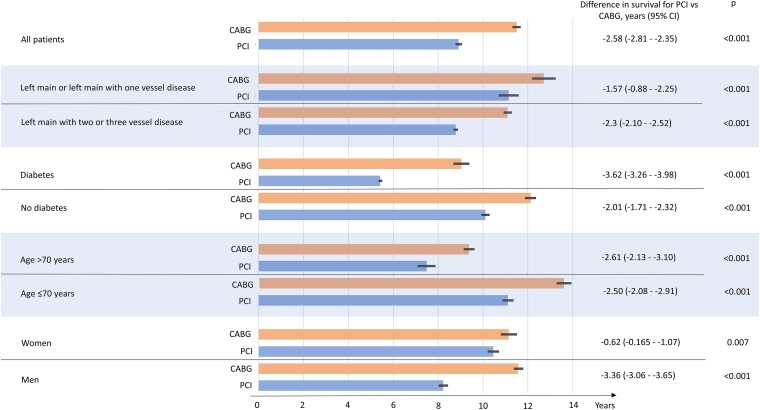
Methods and results: All patients undergoing coronary angiography in Sweden are registered in the Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies registry. Between 01/01/2005 and 12/31/2015, 11 137 patients with LMCA disease underwent CABG (n = 9364) or PCI (n = 1773). Patients with previous CABG, ST-elevation myocardial infarction (MI) or cardiac shock were excluded. Death, MI, stroke, and new revascularization during follow-up until 12/31/2015 were identified using national registries. Cox regression with inverse probability weighting (IPW) and an instrumental variable (IV), administrative region, were used. Patients undergoing PCI were older, had higher prevalence of comorbidity but lower prevalence of three-vessel disease. PCI patients had higher mortality than CABG patients after adjustments for known cofounders with IPW analysis (hazard ratio [HR] 2.0 [95% confidence interval (CI) 1.5-2.7]) and known/unknown confounders with IV analysis (HR 1.5 [95% CI 1.1-2.0]). PCI was associated with higher incidence of major adverse cardiovascular and cerebrovascular events (MACCE; death, MI, stroke, or new revascularization) than CABG, with IV analysis (HR 2.8 [95% CI 1.8-4.5]). There was a quantitative interaction for diabetic status regarding mortality (P = 0.014) translating into 3.6 years (95% CI 3.3-4.0) longer median survival time favouring CABG in patients with diabetes.
Conclusion: In this non-randomized study, CABG in patients with LMCA disease was associated with lower mortality and fewer MACCE compared to PCI after multivariable adjustment for known and unknown confounders.
Keywords: Coronary artery bypass grafting; Cox regression; Instrumental variable analysis; Left main coronary artery disease; Mortality; Percutaneous coronary intervention.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest J.P. has received unrestricted grants from Abbott Inc., unrelated to the present work. J.Y. has no conflicts of interest. O.A. has received research grant and lecture fees from Abbott Inc. D.V. has no conflicts of interest. A.J. has received fees for consultancy or lectures from AstraZeneca, Werfen, Portola, Baxter and LFB Biotechnologies, all unrelated to the present work. I.S. has no conflicts of interest. R.L. has no conflicts of interest. D.E. has no conflicts of interest. T.I. has no conflicts of interest. E.O. has no conflicts of interest.
Figures





Comment in
-
How to treat left main coronary artery disease: the complementary lessons from trials and registries.Eur Heart J. 2023 Aug 7;44(30):2843-2845. doi: 10.1093/eurheartj/ehad287. Eur Heart J. 2023. PMID: 37309774 No abstract available.
-
Observational studies are needed to complete the body of evidence for left main coronary artery disease revascularization strategies.Eur Heart J. 2023 Dec 7;44(46):4894. doi: 10.1093/eurheartj/ehad693. Eur Heart J. 2023. PMID: 37897351 Free PMC article. No abstract available.
References
-
- Yusuf S, Zucker D, Peduzzi P, Fisher LD, Takaro T, Kennedy JW, et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the coronary artery bypass graft surgery trialists collaboration. Lancet 1994;344:563–570. 10.1016/s0140-6736(94)91963-1 - DOI - PubMed
-
- Sianos G, Morel MA, Kappetein AP, Morice MC, Colombo A, Dawkins K, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention 2005;1:219–227. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
