

Neurodegeneration in the retina of motoneuron diseases: a longitudinal study in amyotrophic lateral sclerosis and Kennedy's disease
- PMID: 37289322
- PMCID: PMC10421755
- DOI: 10.1007/s00415-023-11802-2
Neurodegeneration in the retina of motoneuron diseases: a longitudinal study in amyotrophic lateral sclerosis and Kennedy's disease
Abstract
Background: To what extent retinal atrophy in neurodegenerative diseases reflects the severity and/or the chronicity of brain pathology or is a local independent phenomenon remains to be clarified. Moreover, whether retinal atrophy has a clinical (diagnostic and prognostic) value in these diseases remains unclear.
Objective: To add light on the pathological significance and clinical value of retinal atrophy in patients with amyotrophic lateral sclerosis (ALS) and Kennedy's disease (KD).
Methods: Thirty-five ALS, thirty-seven KD, and forty-nine age-matched healthy controls (HC) were included in a one-year longitudinal study. Spectrum-domain optical coherence tomography (OCT) was performed at study entry (T0) and after 12 months (T1). Disease duration and functional rating scale (FRS) for ALS and KD patients were correlated to retinal thicknesses.
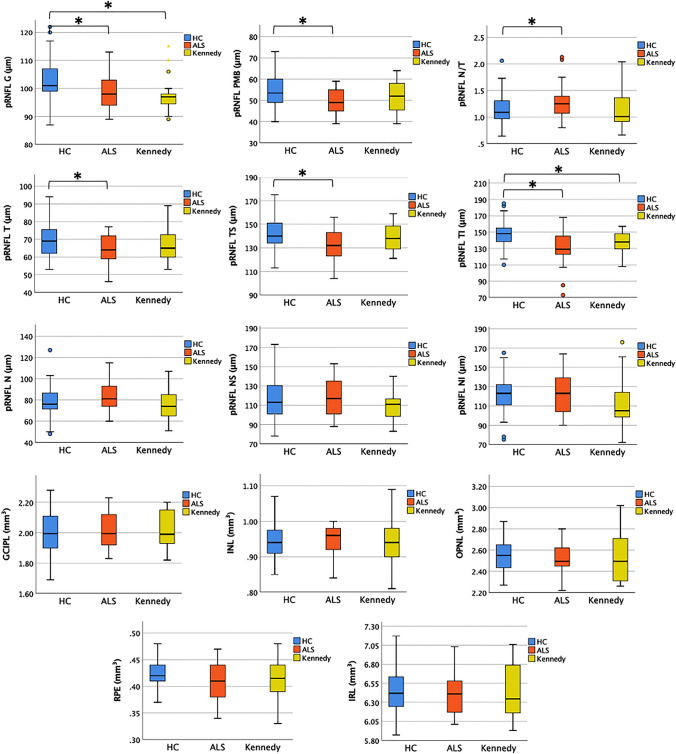
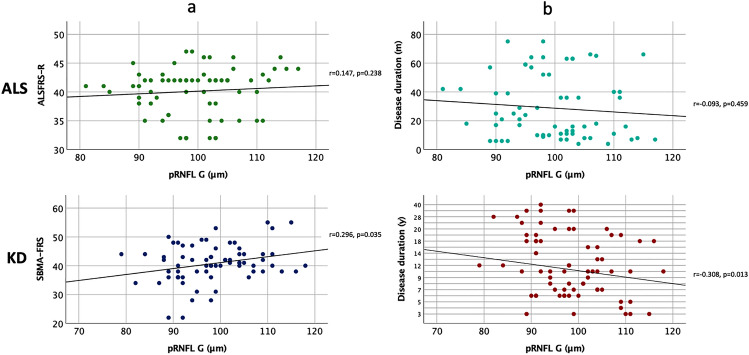
Results: Compared to HC, peripapillary retinal nerve fiber layer (pRNFL) thickness was significantly thinner in both ALS (p = 0.034) and KD (p = 0.003). pRNFL was thinner in KD compared to ALS, but the difference was not significant. In KD, pRNFL atrophy significantly correlated with both disease severity (r = 0.296, p = 0.035) and disease duration (r = - 0.308, p = 0.013) while no significant correlation was found in ALS (disease severity: r = 0.147, p = 0.238; disease duration: r = - 0.093, p = 0.459). During the follow-up, pRNFL thickness remained stable in KD while significantly decreased in ALS (p = 0.043).
Conclusions: Our study provides evidence of retinal atrophy in both ALS and KD and suggests that retinal thinning is a primary local phenomenon in motoneuron diseases. The clinical value of pRNFL atrophy in KD is worthy of further investigation.
Keywords: Amyotrophic lateral sclerosis; Biomarker; Kennedy’s disease; Motoneuron disease; Neurodegeneration; Optical coherence tomography.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Retinal thinning in amyotrophic lateral sclerosis patients without ophthalmic disease.PLoS One. 2017 Sep 25;12(9):e0185242. doi: 10.1371/journal.pone.0185242. eCollection 2017. PLoS One. 2017. PMID: 28945811 Free PMC article.
-
Predictors of retinal atrophy in multiple sclerosis: A longitudinal study using spectral domain optical coherence tomography with segmentation analysis.Mult Scler Relat Disord. 2018 Apr;21:56-62. doi: 10.1016/j.msard.2018.02.010. Epub 2018 Feb 11. Mult Scler Relat Disord. 2018. PMID: 29459346
-
Brain MRI shows white matter sparing in Kennedy's disease and slow-progressing lower motor neuron disease.Hum Brain Mapp. 2019 Jul;40(10):3102-3112. doi: 10.1002/hbm.24583. Epub 2019 Mar 28. Hum Brain Mapp. 2019. PMID: 30924230 Free PMC article.
-
Retinal changes in amyotrophic lateral sclerosis: looking at the disease through a new window.J Neurol. 2021 Jun;268(6):2083-2089. doi: 10.1007/s00415-019-09654-w. Epub 2019 Dec 2. J Neurol. 2021. PMID: 31792674 Review.
-
Optical coherence tomography as a prognostic tool for disability progression in MS: a systematic review.J Neurol. 2023 Feb;270(2):1178-1186. doi: 10.1007/s00415-022-11474-4. Epub 2022 Nov 13. J Neurol. 2023. PMID: 36372866
Cited by
-
Retinal imaging and tissue analysis for frontotemporal degeneration: recent advances and challenges for biomarker development.J Neurol Neurosurg Psychiatry. 2025 Jun 6:jnnp-2024-335723. doi: 10.1136/jnnp-2024-335723. Online ahead of print. J Neurol Neurosurg Psychiatry. 2025. PMID: 40480806 Free PMC article. Review.
-
Longitudinal Changes in the Retinal Nerve Fiber Layer Thickness in Amyotrophic Lateral Sclerosis and Parkinson's Disease.J Clin Neurol. 2024 May;20(3):285-292. doi: 10.3988/jcn.2023.0353. Epub 2024 Apr 2. J Clin Neurol. 2024. PMID: 38627230 Free PMC article.
-
Update on recent advances in amyotrophic lateral sclerosis.J Neurol. 2024 Jul;271(7):4693-4723. doi: 10.1007/s00415-024-12435-9. Epub 2024 May 27. J Neurol. 2024. PMID: 38802624 Free PMC article. Review.
-
Exploring amyotrophic lateral sclerosis through the visual system: A systematic review.Eur J Neurol. 2024 Dec;31(12):e16475. doi: 10.1111/ene.16475. Epub 2024 Sep 20. Eur J Neurol. 2024. PMID: 39302063 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
