

Pregnancy as an Early Cardiovascular Moment: Peripartum Cardiovascular Health
- PMID: 37289905
- PMCID: PMC10254079
- DOI: 10.1161/CIRCRESAHA.123.322001
Pregnancy as an Early Cardiovascular Moment: Peripartum Cardiovascular Health
Abstract
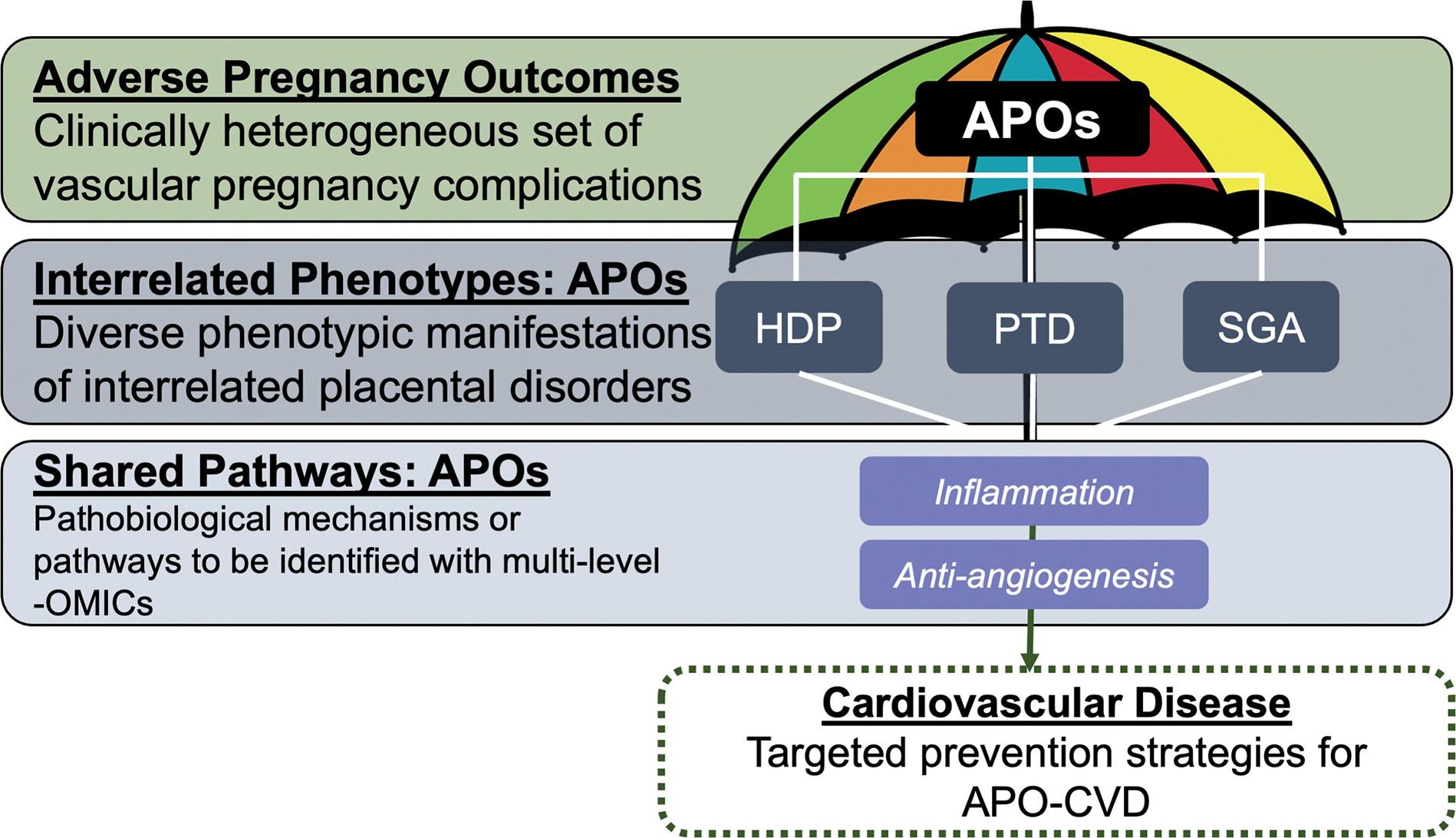
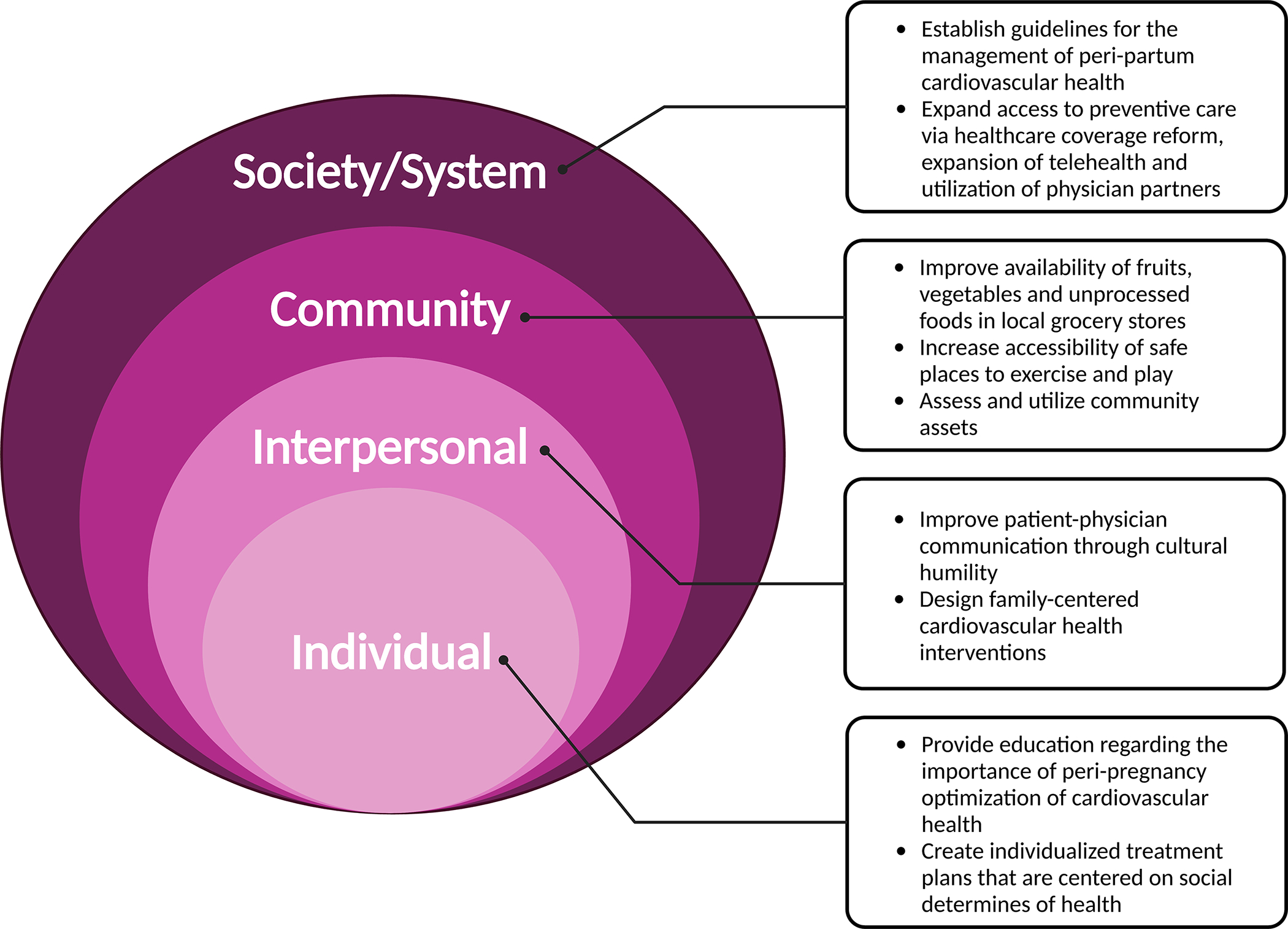
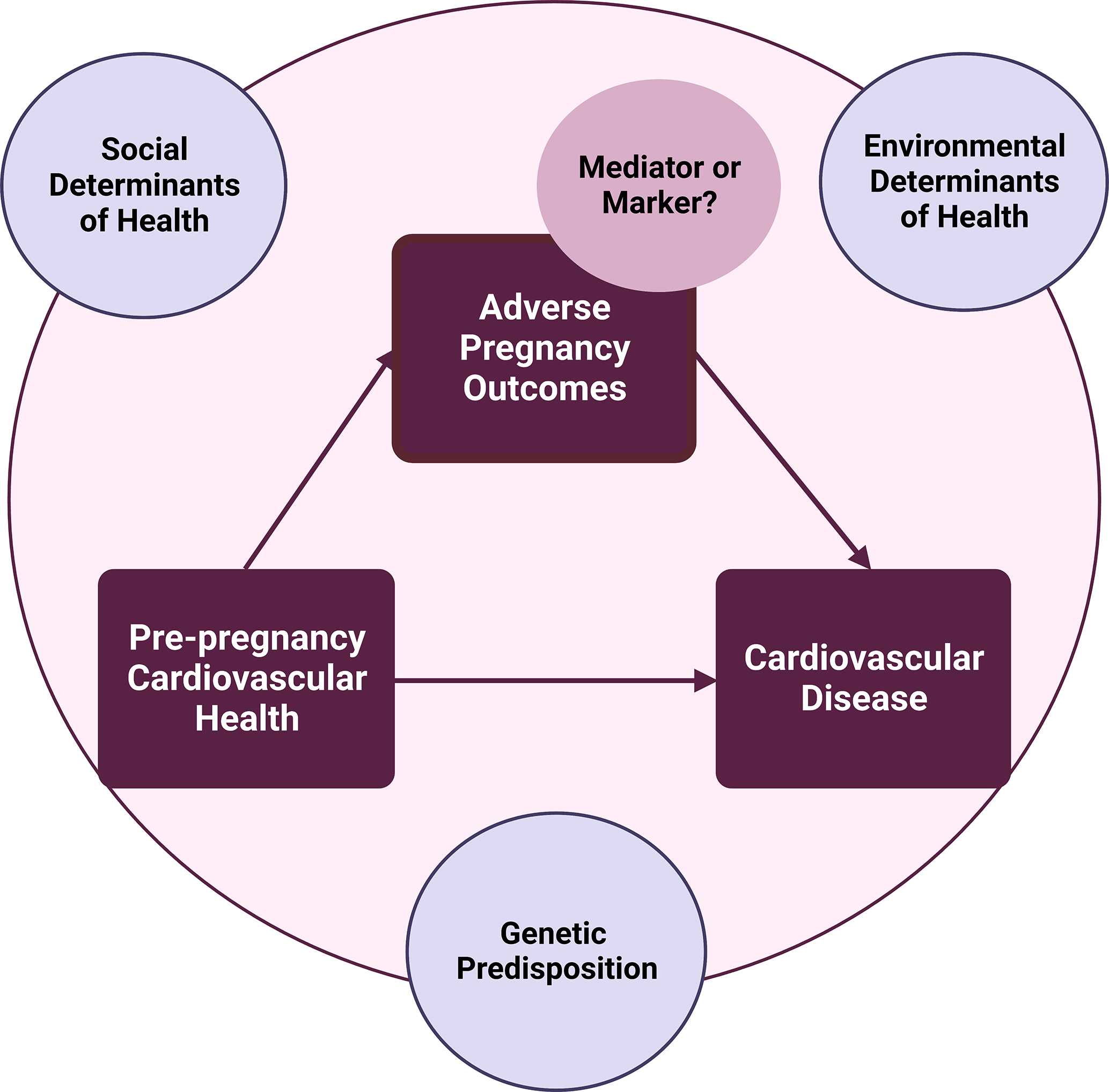
Pregnancy is commonly referred to as a window into future CVH (cardiovascular health). During pregnancy, physiological adaptations occur to promote the optimal growth and development of the fetus. However, in approximately 20% of pregnant individuals, these perturbations result in cardiovascular and metabolic complications, which include hypertensive disorders of pregnancy, gestational diabetes, preterm birth, and small-for-gestational age infant. The biological processes that lead to adverse pregnancy outcomes begin before pregnancy with higher risk of adverse pregnancy outcomes observed among those with poor prepregnancy CVH. Individuals who experience adverse pregnancy outcomes are also at higher risk of subsequent development of cardiovascular disease, which is largely explained by the interim development of traditional risk factors, such as hypertension and diabetes. Therefore, the peripartum period, which includes the period before (prepregnancy), during, and after pregnancy (postpartum), represents an early cardiovascular moment or window of opportunity when CVH should be measured, monitored, and modified (if needed). However, it remains unclear whether adverse pregnancy outcomes reflect latent risk for cardiovascular disease that is unmasked in pregnancy or if adverse pregnancy outcomes are themselves an independent and causal risk factor for future cardiovascular disease. Understanding the pathophysiologic mechanisms and pathways linking prepregnancy CVH, adverse pregnancy outcomes, and cardiovascular disease are necessary to develop strategies tailored for each stage in the peripartum period. Emerging evidence suggests the utility of subclinical cardiovascular disease screening with biomarkers (eg, natriuretic peptides) or imaging (eg, computed tomography for coronary artery calcium or echocardiography for adverse cardiac remodeling) to identify risk-enriched postpartum populations and target for more intensive strategies with health behavior interventions or pharmacological treatments. However, evidence-based guidelines focused on adults with a history of adverse pregnancy outcomes are needed to prioritize the prevention of cardiovascular disease during the reproductive years and beyond.
Keywords: cardiovascular diseases; cardiovascular health; pregnancy; risk factors; women.
Conflict of interest statement
Figures

References
-
- Petersen EE, Davis NL, Goodman D, Cox S, Mayes N, Johnston E, Syverson C, Seed K, Shapiro-Mendoza CK, Callaghan WM, et al. Vital Signs: Pregnancy-Related Deaths, United States, 2011–2015, and Strategies for Prevention, 13 States, 2013–2017. MMWR Morb Mortal Wkly Rep. 2019;68:423–429. doi: 10.15585/mmwr.mm6818e1 - DOI - PMC - PubMed
-
- Hoyert DL. Maternal mortality rates in the United States, 2020. 2022.
-
- Grandi SM, Filion KB, Yoon S, Ayele HT, Doyle CM, Hutcheon JA, Smith GN, Gore GC, Ray JG, Nerenberg K, et al. Cardiovascular Disease-Related Morbidity and Mortality in Women With a History of Pregnancy Complications. Circulation. 2019;139:1069–1079. doi: 10.1161/circulationaha.118.036748 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
