

Development and validation of an international preoperative risk assessment model for postoperative delirium
- PMID: 37290122
- PMCID: PMC10250022
- DOI: 10.1093/ageing/afad086
Development and validation of an international preoperative risk assessment model for postoperative delirium
Abstract
Background: Postoperative delirium (POD) is a frequent complication in older adults, characterised by disturbances in attention, awareness and cognition, and associated with prolonged hospitalisation, poor functional recovery, cognitive decline, long-term dementia and increased mortality. Early identification of patients at risk of POD can considerably aid prevention.
Methods: We have developed a preoperative POD risk prediction algorithm using data from eight studies identified during a systematic review and providing individual-level data. Ten-fold cross-validation was used for predictor selection and internal validation of the final penalised logistic regression model. The external validation used data from university hospitals in Switzerland and Germany.
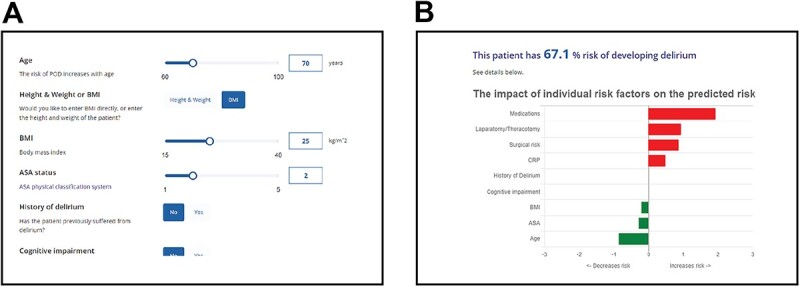
Results: Development included 2,250 surgical (excluding cardiac and intracranial) patients 60 years of age or older, 444 of whom developed POD. The final model included age, body mass index, American Society of Anaesthesiologists (ASA) score, history of delirium, cognitive impairment, medications, optional C-reactive protein (CRP), surgical risk and whether the operation is a laparotomy/thoracotomy. At internal validation, the algorithm had an AUC of 0.80 (95% CI: 0.77-0.82) with CRP and 0.79 (95% CI: 0.77-0.82) without CRP. The external validation consisted of 359 patients, 87 of whom developed POD. The external validation yielded an AUC of 0.74 (95% CI: 0.68-0.80).
Conclusions: The algorithm is named PIPRA (Pre-Interventional Preventive Risk Assessment), has European conformity (ce) certification, is available at http://pipra.ch/ and is accepted for clinical use. It can be used to optimise patient care and prioritise interventions for vulnerable patients and presents an effective way to implement POD prevention strategies in clinical practice.
Keywords: algorithm; clinical practice; older people; postoperative delirium; risk prediction.
© The Author(s) 2023. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
NG has received consultancy fees from PIPRA AG (Zurich, Switzerland). BTD and NSG are founders and employees of PIPRA AG. LF was an employee of PIPRA AG (Zurich, Switzerland). BTD, NSG, LF and NG are shareholders of PIPRA AG. The remaining authors have no conflicts of interest to disclose.
Figures



References
-
- Bickel H, Gradinger R, Kochs E, Förstl H. High risk of cognitive and functional decline after postoperative delirium. Dement Geriatr Cogn Disord 2008; 26: 26–31 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
