

Rituximab De-escalation in Patients With Neuromyelitis Optica Spectrum Disorder
- PMID: 37290967
- PMCID: PMC10435052
- DOI: 10.1212/WNL.0000000000207443
Rituximab De-escalation in Patients With Neuromyelitis Optica Spectrum Disorder
Abstract
Background and objectives: Exit strategies such as de-escalations have not been evaluated for rituximab in patients with neuromyelitis optica spectrum disorder (NMOSD). We hypothesized that they are associated with disease reactivations and aimed to estimate this risk.
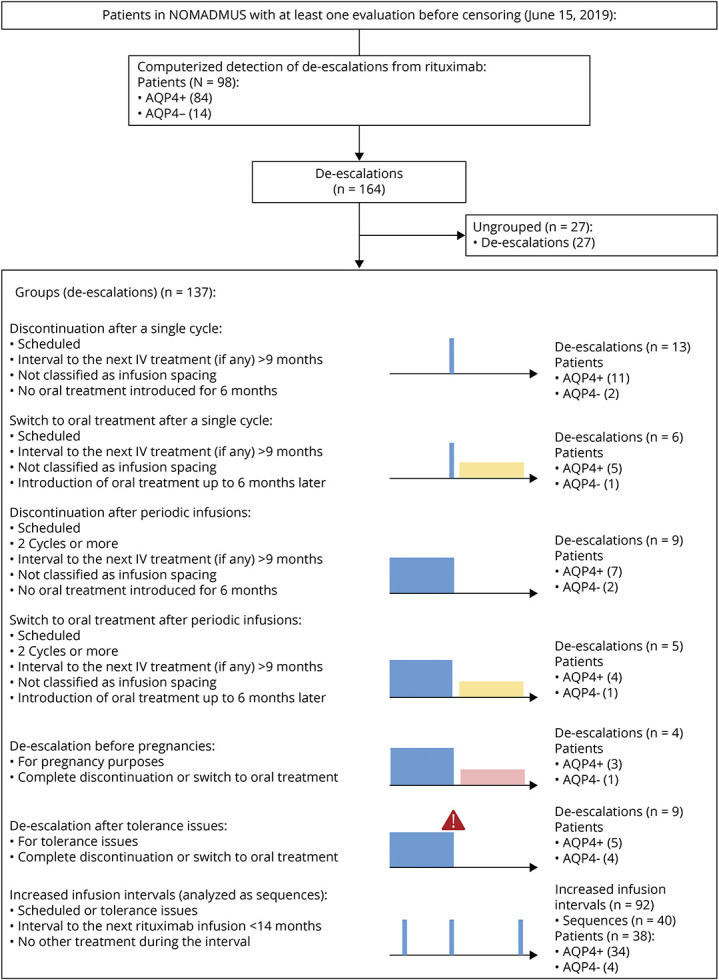
Methods: We describe a case series of real-world de-escalations from the French NMOSD registry (NOMADMUS). All patients met the 2015 International Panel for NMO Diagnosis (IPND) diagnostic criteria for NMOSD. A computerized screening of the registry extracted patients with rituximab de-escalations and at least 12 months of subsequent follow-up. We searched for 7 de-escalation regimens: scheduled discontinuations or switches to an oral treatment after single infusion cycles, scheduled discontinuations or switches to an oral treatment after periodic infusions, de-escalations before pregnancies, de-escalations after tolerance issues, and increased infusion intervals. Rituximab discontinuations motivated by inefficacy or for unknown purposes were excluded. The primary outcome was the absolute risk of NMOSD reactivation (one or more relapses) at 12 months. AQP4+ and AQP4- serotypes were analyzed separately.
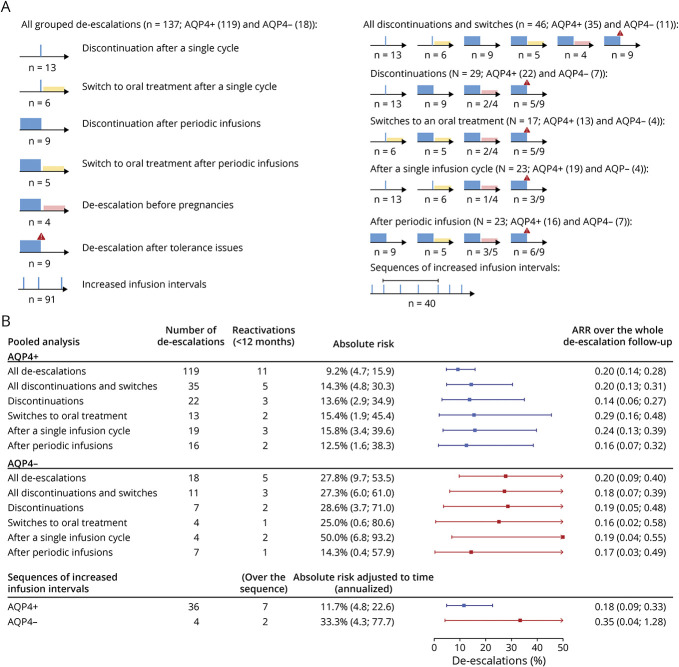
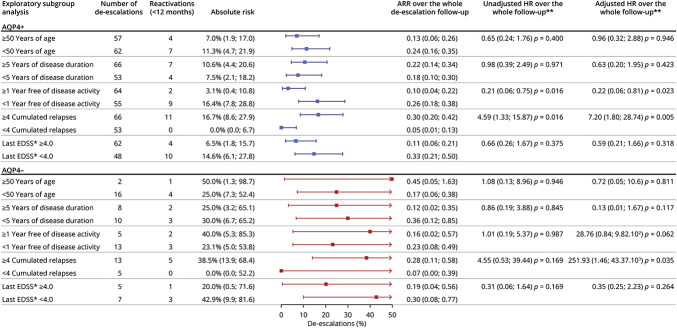
Results: We identified 137 rituximab de-escalations between 2006 and 2019 that corresponded to a predefined group: 13 discontinuations after a single infusion cycle, 6 switches to an oral treatment after a single infusion cycle, 9 discontinuations after periodic infusions, 5 switches to an oral treatment after periodic infusions, 4 de-escalations before pregnancies, 9 de-escalations after tolerance issues, and 91 increased infusion intervals. No group remained relapse-free over the whole de-escalation follow-up (mean: 3.2 years; range: 0.79-9.5), except pregnancies in AQP+ patients. In all groups combined and within 12 months, reactivations occurred after 11/119 de-escalations in patients with AQP4+ NMOSD (9.2%, 95% CI [4.7-15.9]), from 0.69 to 10.0 months, and in 5/18 de-escalations in patients with AQP4- NMOSD (27.8%, 95% CI [9.7-53.5]), from 1.1 to 9.9 months.
Discussion: There is a risk of NMOSD reactivation whatever the rituximab de-escalation regimen.
Trial registration information: Registered on ClinicalTrials.gov: NCT02850705.
Classification of evidence: This study provides Class IV evidence that de-escalation of rituximab increases the probability of disease reactivation.
© 2023 American Academy of Neurology.
Conflict of interest statement
S. Demuth reports no disclosures. N. Collongues has received honoraria for consulting or presentation from Biogen Idec, Alexion, Novartis, Merck Serono, Bristol-Myers Squibb, Sanofi-Genzyme, and Roche, and is a member of the Editorial Board of the Journal de la Ligue Française contre la Sclérose en plaques. B. Audoin, X. Ayrignac, B. Bourre report no disclosures. J. Ciron has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with Biogen, Novartis, Merck, Sanofi-Genzyme, Roche, Celgene-BMS, Alexion, none related to this study. M. Cohen has received honorarium for participating on scientific advisory boards for Ad Scientiam, Alexion, Biogen, BMS, Horizon therapeutics, Merck, Novartis, Roche, and Teva. R. Deschamps, F. Durand Dubief report no disclosures. E. Maillart reports personal fees from Alexion, Biogen, Merck, Novartis, Roche, Sanofi, and Teva, and grants from Biogen, outside the submitted work. C. Papeix reports no disclosures. A. Ruet reports personal fees and research grants from Biogen, personal fees and research grant from Roche, research grant from Genzyme, personal fees and research grant from Merck, research grant from Bayer, outside the submitted work. H. Zéphir has received consulting fees from Biogen Idec, Roche, Alexion, BMS, Sanofi, Merck, and Novartis but reports no disclosures directly related to the manuscript. R. Marignier serves on the scientific advisory board for Viela Bio, Roche, UCB, and Alexion, and has received honoraria from Biogen, Merck, and Novartis. J. de Seze reports no disclosures. Go to
Figures
Comment in
-
Treatment De-escalation in AQP4-Ab Neuromyelitis Optica Spectrum Disorder.Neurology. 2023 Jul 25;101(4):153-154. doi: 10.1212/WNL.0000000000207521. Epub 2023 Jun 13. Neurology. 2023. PMID: 37311650 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous