

Prognostic Language in Critical Neurologic Illness: A Multicenter Mixed-Methods Study
- PMID: 37290972
- PMCID: PMC10401677
- DOI: 10.1212/WNL.0000000000207462
Prognostic Language in Critical Neurologic Illness: A Multicenter Mixed-Methods Study
Abstract
Background and objectives: There are no evidence-based guidelines for discussing prognosis in critical neurologic illness, but in general, experts recommend that clinicians communicate prognosis using estimates, such as numerical or qualitative expressions of risk. Little is known about how real-world clinicians communicate prognosis in critical neurologic illness. Our primary objective was to characterize prognostic language clinicians used in critical neurologic illness. We additionally explored whether prognostic language differed between prognostic domains (e.g., survival, cognition).
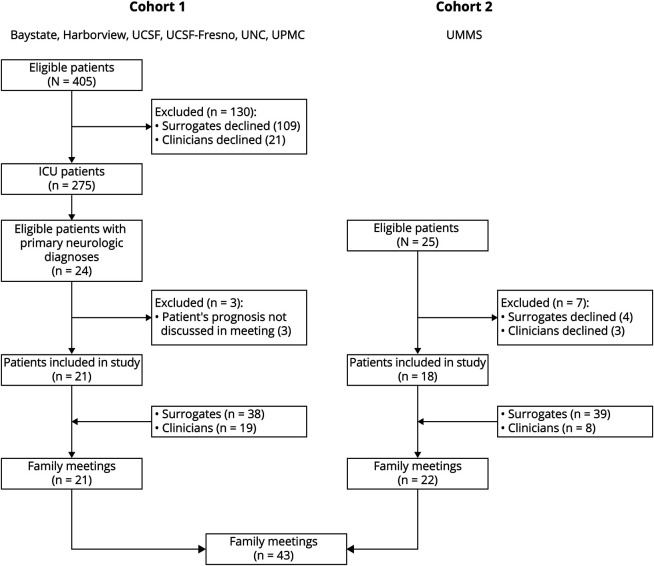
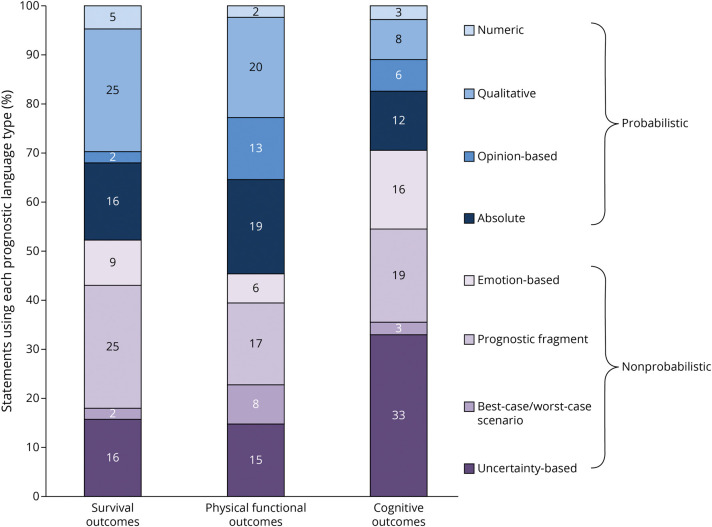
Methods: We conducted a multicenter cross-sectional mixed-methods study analyzing deidentified transcripts of audio-recorded clinician-family meetings for patients with neurologic illness requiring intensive care (e.g., intracerebral hemorrhage, traumatic brain injury, severe stroke) from 7 US centers. Two coders assigned codes for prognostic language type and domain of prognosis to each clinician prognostic statement. Prognostic language was coded as probabilistic (estimating the likelihood of an outcome occurring, e.g., "80% survival"; "She'll probably survive") or nonprobabilistic (characterizing outcomes without offering likelihood; e.g., "She may not survive"). We applied univariate and multivariate binomial logistic regression to examine independent associations between prognostic language and domain of prognosis.
Results: We analyzed 43 clinician-family meetings for 39 patients with 78 surrogates and 27 clinicians. Clinicians made 512 statements about survival (median 0/meeting [interquartile range (IQR) 0-2]), physical function (median 2 [IQR 0-7]), cognition (median 2 [IQR 0-6]), and overall recovery (median 2 [IQR 1-4]). Most statements were nonprobabilistic (316/512 [62%]); 10 of 512 prognostic statements (2%) offered numeric estimates; and 21% (9/43) of family meetings only contained nonprobabilistic language. Compared with statements about cognition, statements about survival (odds ratio [OR] 2.50, 95% CI 1.01-6.18, p = 0.048) and physical function (OR 3.22, 95% 1.77-5.86, p < 0.001) were more frequently probabilistic. Statements about physical function were less likely to be uncertainty-based than statements about cognition (OR 0.34, 95% CI 0.17-0.66, p = 0.002).
Discussion: Clinicians preferred not to use estimates (either numeric or qualitative) when discussing critical neurologic illness prognosis, especially when they discussed cognitive outcomes. These findings may inform interventions to improve prognostic communication in critical neurologic illness.
© 2023 American Academy of Neurology.
Conflict of interest statement
A.L. Goss reports no disclosures relevant to the manuscript. C. Ge was funded by the American Academy of Neurology Medical Student Research Scholarship (2020). S. Crawford, K. Goostrey, and P. Buddadhumaruk report no disclosures relevant to the manuscript. C.L. Hough is supported by K24HL141526 and the American Lung Association through payments to her institution. She receives consulting fees from Quantum Leap and the NIH. She receives support for attending Critical Care Reviews meetings. She participates on advisory boards for the NIH, Quantum Leap, and ANSICS. B. Lo receives royalties from Wolters Kluwer for his book, Resolving Ethical Dilemmas. S. Carson reports no disclosures relevant to the manuscript. J. Steingrub reports no disclosures relevant to the manuscript. D.B. White was funded NIH-NHLBI: K24HL148314. Collection of data occurred under the parent ECALI R01, NIH-NHLBI 5R01HL094553. S. Muehlschlegel's research time was funded by NIH/NICHD K23HD080971 and NIH/NINR R21NR020231. Go to
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources