

Signaling-specific inhibition of the CB1 receptor for cannabis use disorder: phase 1 and phase 2a randomized trials
- PMID: 37291212
- PMCID: PMC10287566
- DOI: 10.1038/s41591-023-02381-w
Signaling-specific inhibition of the CB1 receptor for cannabis use disorder: phase 1 and phase 2a randomized trials
Abstract
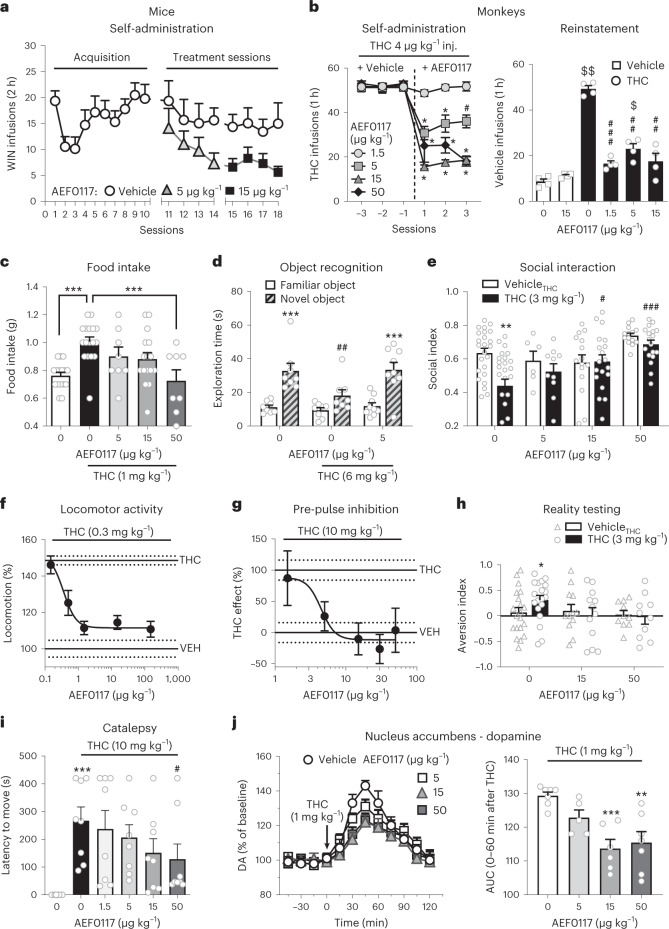
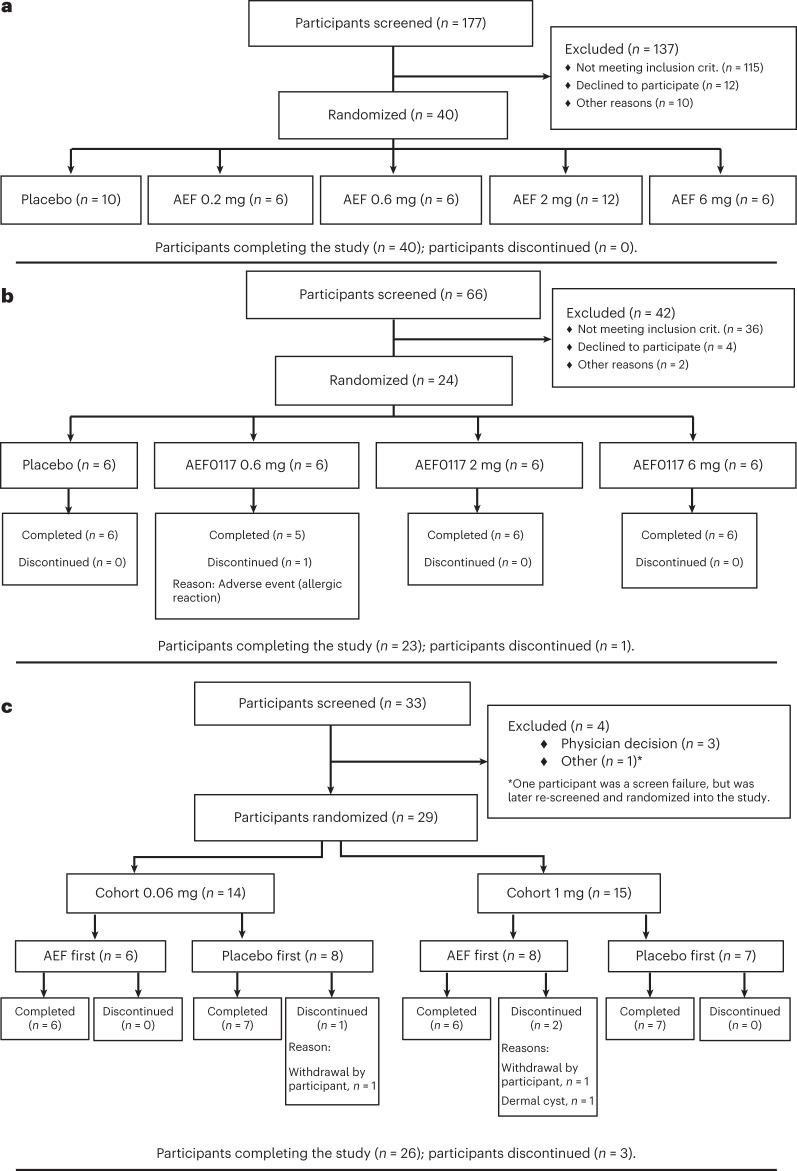
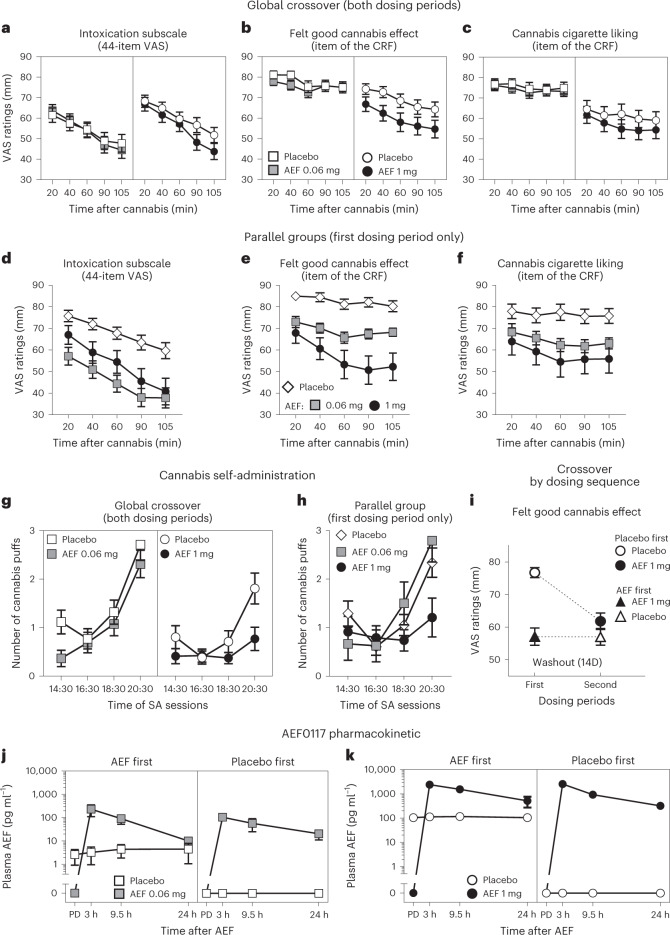
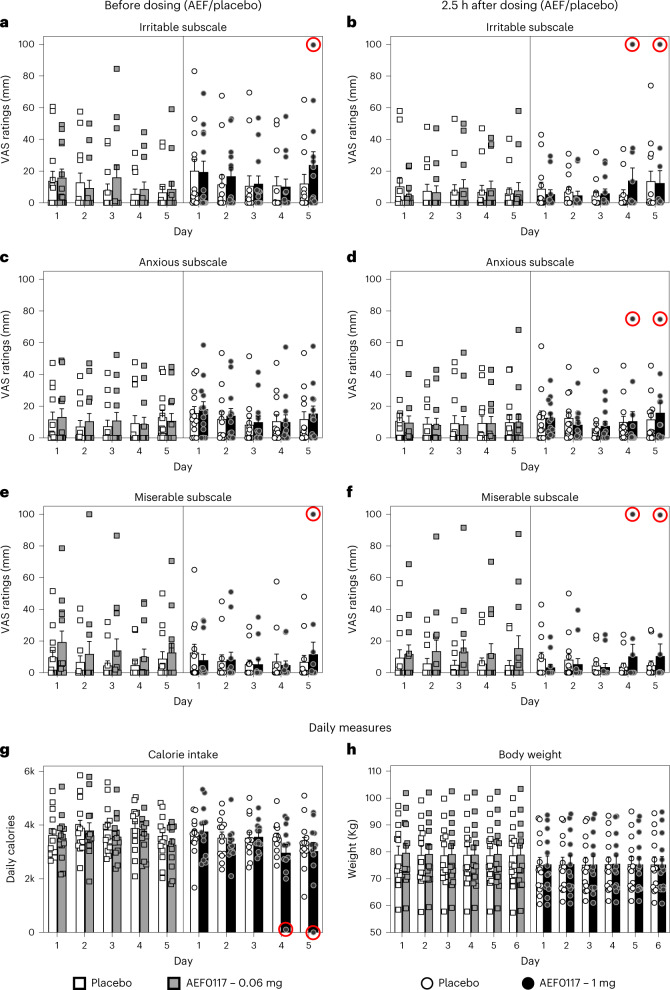
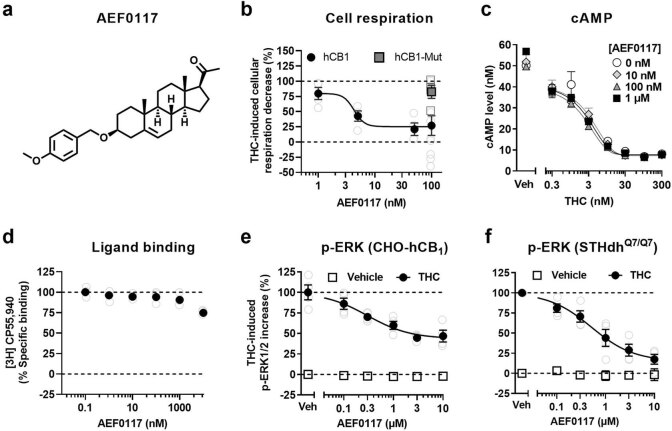
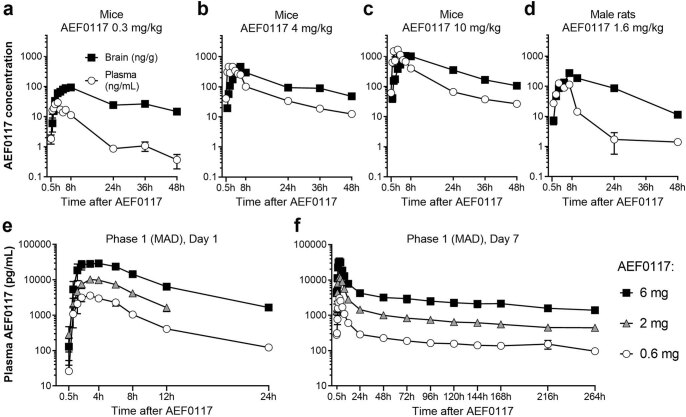
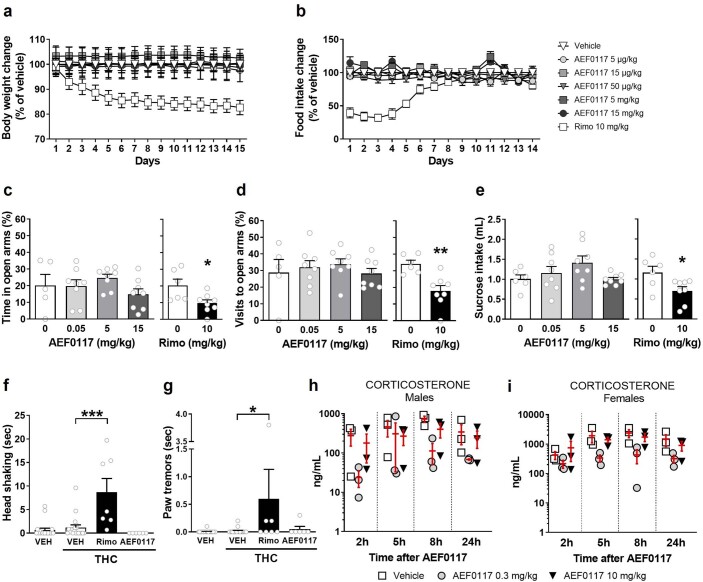
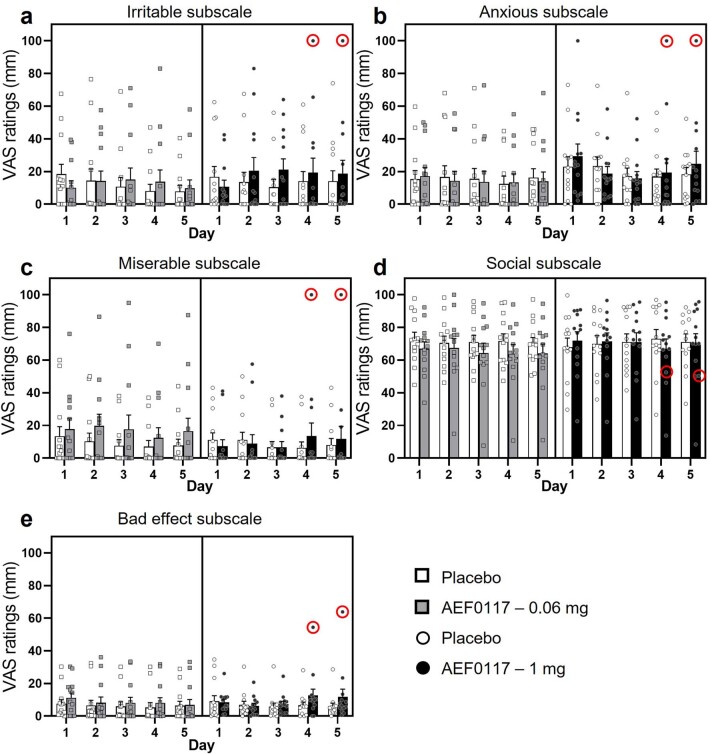
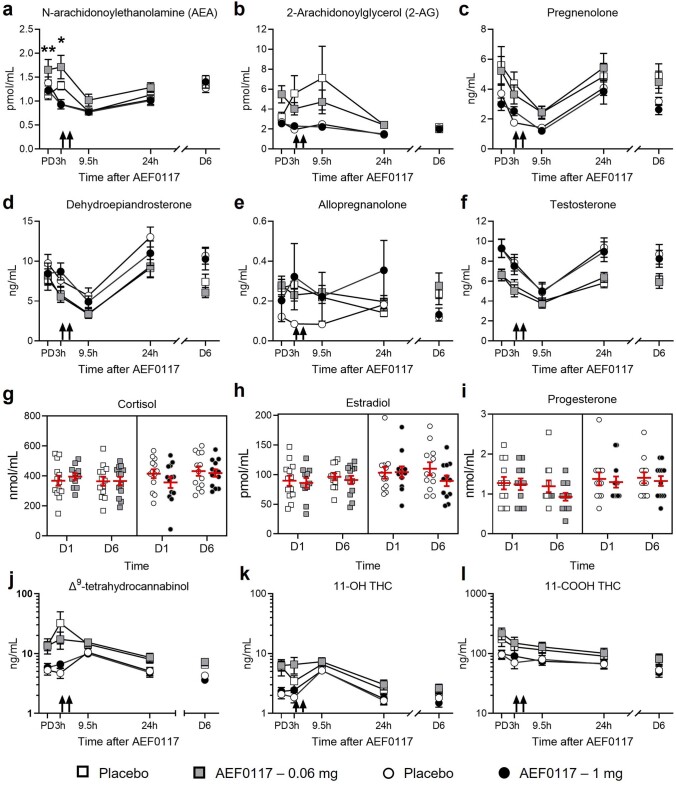
Cannabis use disorder (CUD) is widespread, and there is no pharmacotherapy to facilitate its treatment. AEF0117, the first of a new pharmacological class, is a signaling-specific inhibitor of the cannabinoid receptor 1 (CB1-SSi). AEF0117 selectively inhibits a subset of intracellular effects resulting from Δ9-tetrahydrocannabinol (THC) binding without modifying behavior per se. In mice and non-human primates, AEF0117 decreased cannabinoid self-administration and THC-related behavioral impairment without producing significant adverse effects. In single-ascending-dose (0.2 mg, 0.6 mg, 2 mg and 6 mg; n = 40) and multiple-ascending-dose (0.6 mg, 2 mg and 6 mg; n = 24) phase 1 trials, healthy volunteers were randomized to ascending-dose cohorts (n = 8 per cohort; 6:2 AEF0117 to placebo randomization). In both studies, AEF0117 was safe and well tolerated (primary outcome measurements). In a double-blind, placebo-controlled, crossover phase 2a trial, volunteers with CUD were randomized to two ascending-dose cohorts (0.06 mg, n = 14; 1 mg, n = 15). AEF0117 significantly reduced cannabis' positive subjective effects (primary outcome measurement, assessed by visual analog scales) by 19% (0.06 mg) and 38% (1 mg) compared to placebo (P < 0.04). AEF0117 (1 mg) also reduced cannabis self-administration (P < 0.05). In volunteers with CUD, AEF0117 was well tolerated and did not precipitate cannabis withdrawal. These data suggest that AEF0117 is a safe and potentially efficacious treatment for CUD.ClinicalTrials.gov identifiers: NCT03325595 , NCT03443895 and NCT03717272 .
© 2023. The Author(s).
Conflict of interest statement
P.V.P., S.M., S.F., M.M., R.M., U.S. and H.M. are stockholders of Aelis Farma. M.V., J.-M.R., D.C. and G.M. are stockholders of and consultants for Aelis Farma. M.Z., G.C., L.L.T., A.B. and R.S. have stock options of Aelis Farma. M.G. is a consultant of Aelis Farma. P.V.P., M.V., F.X.F., J.-M.R. and S.F. are inventors on a composition-of-matter patent application (patent family WO2014/083068) that covers AEF0117. P.P.V., S.F., M.M., S.M., A.B.-G., D.C., G.M., J.-M.R. and M.V. are inventors on a method-of-use patent application (patent family WO2019/162328) that covers use of AEF0117 for the treatment of cannabinoid-related disorders. M.H. is a stockholder and on the Scientific Advisory Board of Pleo Pharma. The remaining authors declare no competing interests.
Figures
Comment in
-
Treating cannabis use disorder.Nat Rev Drug Discov. 2023 Aug;22(8):623. doi: 10.1038/d41573-023-00110-z. Nat Rev Drug Discov. 2023. PMID: 37400710 No abstract available.
References
-
- Substance Abuse and Mental Health Services Administration (SAMSHA). Key substance use and mental health indicators in the United States: results from the 2020 national survey on drug use and health (HHS publication no. PEP21-07-01-003, SAMSHA). https://www.samhsa.gov/data/sites/default/files/reports/rpt35325/NSDUHFF...) (2021).
-
- Substance Abuse and Mental Health Services Administration (SAMSHA). Treatment Episode Data Set (TEDS): 2005–2015 national admissions to substance abuse treatment services (HHS publication no. (SMA) 17-5037, SAMSHA). https://www.samhsa.gov/data/sites/default/files/2015_Treatment_Episode_D... (2017).
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th edn. American Psychiatric Association; 2013.
