

Native T1 high region and left ventricular ejection fraction recovery in patients with dilated cardiomyopathy
- PMID: 37291379
- PMCID: PMC10520178
- DOI: 10.1007/s10554-023-02888-w
Native T1 high region and left ventricular ejection fraction recovery in patients with dilated cardiomyopathy
Abstract
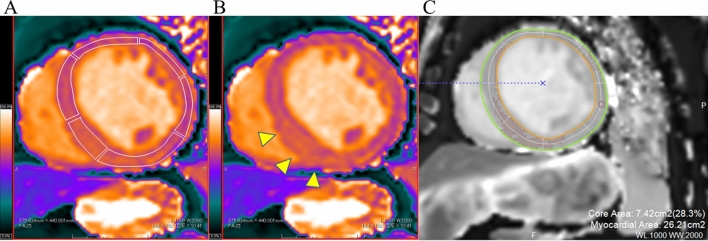
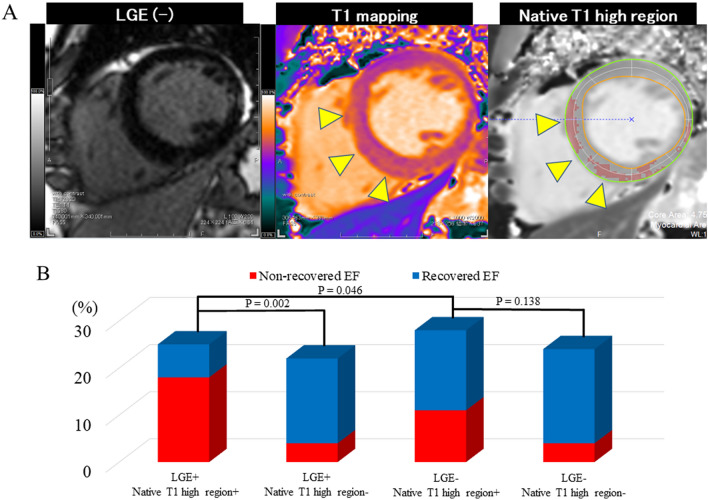
Native T1 mapping is used to assess myocardial tissue characteristics without gadolinium contrast agents. The focal T1 high-intensity region can indicate myocardial alterations. This study aimed to identify the association between the native T1 mapping including the native T1 high region and left ventricular ejection fraction (LVEF) recovery in patients with dilated cardiomyopathy (DCM). Patients with newly diagnosed DCM (LVEF of < 45%) who underwent cardiac magnetic resonance imaging with native T1 mapping were included in the analysis. Native T1 high region was defined as a signal intensity of > 5 SD in the remote myocardium. Recovered EF was defined as a follow-up LVEF of ≥ 45% and an LVEF increase of ≥ 10% after 2 years from baseline. Seventy-one patients met the inclusion criteria for this study. Forty-four patients (61.9%) achieved recovered EF. Logistic regression analysis showed that the native T1 value (OR: 0.98; 95% CI: 0.96-0.99; P = 0.014) and the native T1 high region (OR: 0.17; 95% CI: 0.05-0.55; P = 0.002), but not late gadolinium enhancement, were independent predictors of recovered EF. Compared with native T1 value alone, combined native T1 high region and native T1 value improved the area under the curve from 0.703 to 0.788 for predicting recovered EF. Myocardial damage, which was quantified using native T1 mapping and the native T1 high region were independently associated with recovered EF in patients with newly diagnosed DCM.
Keywords: Cardiac magnetic resonance; Dilated cardiomyopathy; Left ventricular ejection fraction recovery; T1 mapping.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, et al. Classification of the cardiomyopathies: a position statement from the european society of cardiology working group on myocardial and pericardial diseases. Eur Heart J. 2008;29(2):270–276. doi: 10.1093/eurheartj/ehm342. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
