

Clonazepam Loading Dose in Status Epilepticus: Is More Always Better?
- PMID: 37291410
- PMCID: PMC10276784
- DOI: 10.1007/s40263-023-01012-9
Clonazepam Loading Dose in Status Epilepticus: Is More Always Better?
Abstract
Background and objectives: Benzodiazepines are the first treatment line in status epilepticus (SE). Despite their well-established benefit, benzodiazepines are frequently underdosed with potential detrimental consequences. In some European countries, clonazepam (CLZ) is commonly used as the first line treatment. The aim of this study was to explore the correlation between CLZ loading doses and SE outcome.
Methods: This study included a retrospective analysis of a prospective registry in Lausanne, Switzerland (CHUV Lausanne University Hospital), including all SE episodes treated between February 2016 and February 2021. Only adults (> 16 years old) were included with CLZ used as the first treatment line. Post-anoxic SE were excluded because of significant differences in physiopathology and prognosis. Patient characteristics, SE features, the validated SE severity score (STESS), and treatment characteristics were prospectively recorded. We considered loading doses of 0.015 mg/kg or higher (following commonly recommended loading doses) as high doses. We analyzed outcome in terms of number of treatment lines after the CLZ, proportion of refractory episodes, intubation for airways protection, intubation for SE treatment, and mortality. We performed univariable analyses to investigate the association between loading doses and clinical response. A multivariable stepwise backward binary logistic regression was applied for adjusting for potential confounders. Multivariable linear regression was similarly used to analyze CLZ dose as a continuous variable.
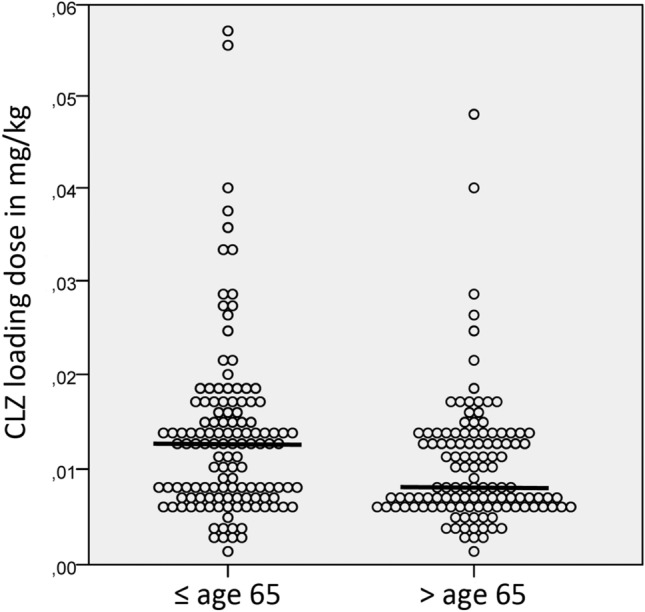
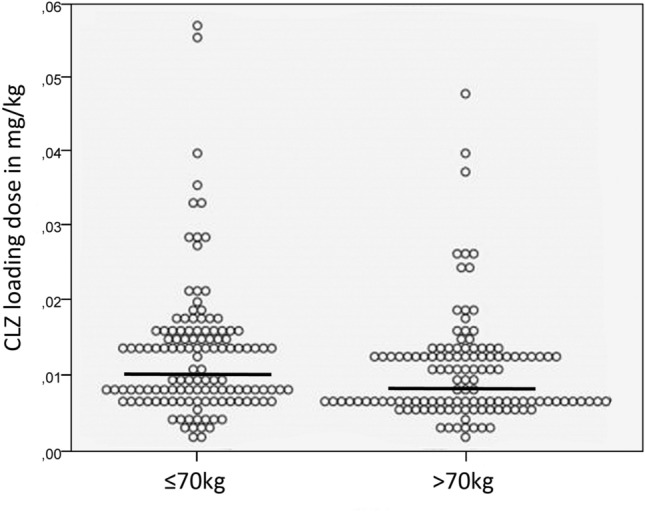
Results: We collected 251 SE episodes in 225 adult patients. Median CLZ loading dose was 0.010 mg/kg. CLZ high doses were used in 21.9% of SE episodes (in 43.8% for > 80% of the high dose). Thirteen percent of patients with SE were intubated for airways control, while intubation was needed in 12.7% for SE treatment. High CLZ loading doses were independently associated with younger age (median 62 versus 68 years old, p = 0.002), lesser weight (65 kg versus 75 kg, p = 0.001) and more frequent intubation for airways protection (23% vs 11%, p = 0.013), but differing CLZ dose was not associated with any outcome parameter.
Conclusion: CLZ high doses were more frequently used for SE treatment in younger patients with healthy weight and were more often associated with intubation for airways protection, probably as an adverse event. Varying CLZ dose did not alter outcome in SE, raising the possibility that commonly recommended doses are above what is needed, at least in some patients. Our results suggest that CLZ doses in SE may be individualized depending on the clinical setting.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Practice variability and efficacy of clonazepam, lorazepam, and midazolam in status epilepticus: A multicenter comparison.Epilepsia. 2015 Aug;56(8):1275-85. doi: 10.1111/epi.13056. Epub 2015 Jul 3. Epilepsia. 2015. PMID: 26140660 Free PMC article.
-
Evaluation of levetiracetam loading dose in adult patients with benzodiazepine-refractory status epilepticus.Am J Emerg Med. 2024 Nov;85:148-152. doi: 10.1016/j.ajem.2024.09.007. Epub 2024 Sep 2. Am J Emerg Med. 2024. PMID: 39270551
-
Refractory Status Epilepticus: Risk Factors and Analysis of Intubation in the Multicenter SENSE Registry.Neurology. 2022 Oct 18;99(16):e1824-e1834. doi: 10.1212/WNL.0000000000201099. Epub 2022 Aug 10. Neurology. 2022. PMID: 35948449
-
Drug Trials in Status Epilepticus: Current Evidence and Future Concepts.J Clin Neurophysiol. 2020 Sep;37(5):434-445. doi: 10.1097/WNP.0000000000000713. J Clin Neurophysiol. 2020. PMID: 32890066 Review.
-
Clonazepam in the treatment of status epilepticus.Expert Rev Neurother. 2015;15(7):733-40. doi: 10.1586/14737175.2015.1056781. Expert Rev Neurother. 2015. PMID: 26109227 Review.
References
-
- Navarro V, Dagron C, Elie C, Lamhaut L, Demeret S, Urien S, et al. Prehospital treatment with levetiracetam plus clonazepam or placebo plus clonazepam in status epilepticus (SAMUKeppra): a randomised, double-blind, phase 3 trial. Lancet Neurol. 2016;15(1):47–55. doi: 10.1016/S1474-4422(15)00296-3. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
