

Comparative evaluation of clinical and cerebrospinal fluid biomarker characteristics in rapidly and non-rapidly progressive Alzheimer's disease
- PMID: 37291640
- PMCID: PMC10249304
- DOI: 10.1186/s13195-023-01249-y
Comparative evaluation of clinical and cerebrospinal fluid biomarker characteristics in rapidly and non-rapidly progressive Alzheimer's disease
Erratum in
-
Correction: Comparative evaluation of clinical and cerebrospinal fluid biomarker characteristics in rapidly and non‑rapidly progressive Alzheimer's disease.Alzheimers Res Ther. 2023 Jun 22;15(1):116. doi: 10.1186/s13195-023-01263-0. Alzheimers Res Ther. 2023. PMID: 37349779 Free PMC article. No abstract available.
Abstract
Background: Rapidly progressive forms of Alzheimer's disease (rpAD) are increasingly recognized and may have a prevalence of up to 30% of patients among all patients with Alzheimer's disease (AD). However, insights about risk factors, underlying pathophysiological processes, and clinical characteristics of rpAD remain controversial. This study aimed to gain a comprehensive picture of rpAD and new insights into the clinical manifestation to enable a better interpretation of disease courses in clinical practice as well as in future clinical studies.
Methods: Patients (n = 228) from a prospective observational study on AD were selected and categorized into rpAD (n = 67) and non-rpAD (n = 161) disease groups. Patients were recruited through the German Creutzfeldt-Jakob disease surveillance center and the memory outpatient clinic of the Göttingen University Medical Center, representing diverse phenotypes of the AD population. Biomarkers and clinical presentation were assessed using standardized protocols. A drop of ≥ MMSE 6 points within 12 months defined rapid progressors.
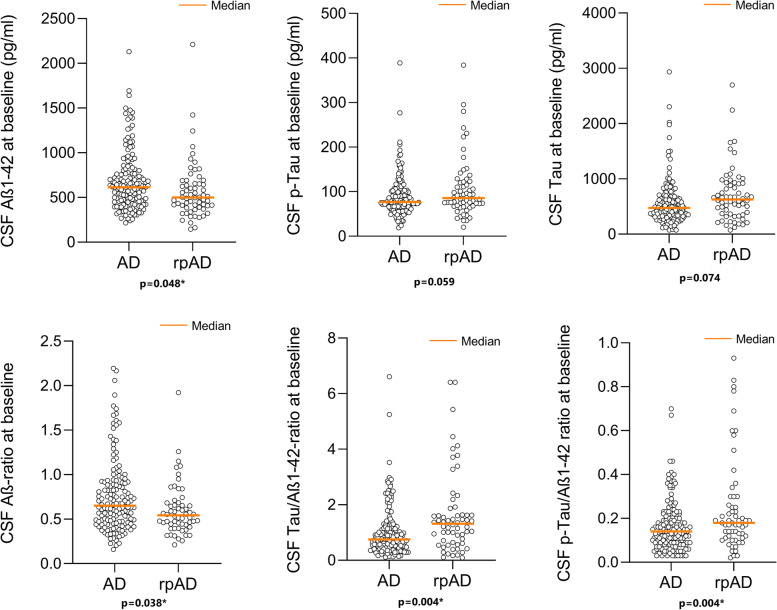
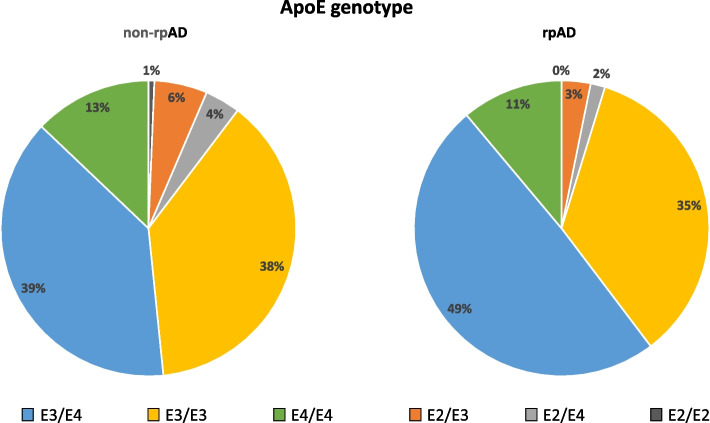
Results: Lower CSF Amyloid beta 1-42 concentrations (p = 0.048), lower Amyloid beta 42/40 ratio (p = 0.038), and higher Tau/Amyloid-beta 1-42 ratio, as well as pTau/Amyloid-beta 1-42 ratio (each p = 0.004) were associated with rpAD. Analyzes in a subset of the cohort (rpAD: n = 12; non-rpAD: n = 31) showed higher CSF NfL levels in rpAD (p = 0.024). Clinically, rpAD showed earlier impairment of functional abilities (p < 0.001) and higher scores on the Unified Parkinson's Disease Rating Scale III (p < 0.001), indicating pronounced extrapyramidal motor symptoms. Furthermore, cognitive profiles (adjusted for overall cognitive performance) indicated marked deficits in semantic (p = 0.008) and phonematic (0.023) verbal fluency tests as well as word list learning (p = 0.007) in rpAD compared to non-rpAD. The distribution of APOE genotypes did not differ significantly between groups.
Conclusions: Our results suggest that rpAD is associated with distinct cognitive profiles, earlier occurrence of non-cognitive symptoms, extrapyramidal motoric disturbance, and lower Amyloid-beta 1-42 concentrations in the CSF. The findings may help to characterize a distinct phenotype of rpAD and estimate prognosis based on clinical characteristics and biomarker results. However, an important future goal should be a unified definition for rpAD to enable targeted study designs and better comparability of the results.
Keywords: APOE; Alzheimer’s disease; Biomarkers; Phenotype; Rapidly progressive Alzheimer’s disease.
© 2023. The Author(s).
Conflict of interest statement
IZ and AVP had received test Kits for the initial t-PrP analyzes without payment from Roboscreen GmbH, Leipzig, Germany (see Reference no. 31). Beside this, JMH, PH, KD, LW, SN, CV, AS, SG, FK, SC, DW, CS, AVP, and IZ have no competing interests to disclose.
Figures
References
-
- Brodaty H, Breteler MM, Dekosky ST, Dorenlot P, Fratiglioni L, Hock C, et al. The world of dementia beyond 2020. J Am Geriatr Soc. 2011;59:923–927. - PubMed
-
- Schmidt C, Redyk K, Meissner B, Krack L, von Ahsen N, Roeber S, et al. Clinical features of rapidly progressive Alzheimer’s disease. Dement Geriatr Cogn Disord Karger Publishers. 2010;29:371–378. - PubMed
-
- Abu-Rumeileh S, Capellari S, Parchi P. Rapidly progressive Alzheimer’s disease: contributions to clinical-pathological definition and diagnosis. J Alzheimers Dis IOS Press. 2018;63:887–897. - PubMed
-
- Schmidt C, Wolff M, Weitz M, Bartlau T, Korth C, Zerr I. Rapidly progressive Alzheimer disease. Arch Neurol. 2011;68:1124–1130. - PubMed
-
- Wallace L, Walsh S, Brayne C. The legacy of the 2013 G8 Dementia Summit: successes, challenges, and potential ways forward. Lancet Healthy Longev Elsevier. 2021;2:e455–e457. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
